Human Rights and the Psychiatric Setting
This is an article exploring human rights in relation to the mental health industrial complex which has risen to articulate the way which people are treated in response to their need for support. In this piece of writing I examine human rights discourses in the context of present day Britain and deconstruct some of the ideological narratives we find intersecting in mental health ultimately asking questions about harms and interrelationships.

Table of Contents
Introduction
The intention of this article is an exploration of different configurations of understanding mental health picking up on cascading possibilities which can impact on individuals in negative ways. Making sense of a highly disputed and conflict riven area of thinking and life itself like mental health is one of the great challenges of our time.
For the last twenty years I have researched biochemistry of various living processes becoming interested in the science by studying things like the production of substances in the body by enzymes and what goes wrong when those enzymes stop doing their job. My research focused over the years many times on understanding physiological causes of altered cognition, memory and affect; for example, how changes in the function of the thyroid can result in psychiatric manifestations.
I continue to research and explore the increasing volume of biochemistry related to the nervous system and the brain and practically every other part of us. The availability of knowledge produced from the academic scientific community is very encouraging for the way that with a computer and the internet you can access a library far exceeding any physical library which could be built practically. Anyone can in principle access a significant amount of robustly done peer reviewed materials on say the myelin sheath which insults the nerve.
Whilst it was my first literacy the more I came to think about and research the field of psychiatry, the more I kept on coming across incidences where there were systems effects in bringing about harms which could not be accounted for through biochemistry models. Critical mental health studies is gaining ground because there has been so much evidence accrued for correctives to be suggested to the existing schemes of thought.

When I say systems effects because there are many different systems which have an effect on the state of someone’s wellbeing. This means that we can only get at certain understandings by employing systems thinking to the study of problems. In part by philosophical evolutions like those suggested by Fritof Capra and Gregory Bateson.

There are no easy answers, and in some cases uncomfortable answers, in any particular enquiry into anthropologically loaded cultural perceptions of what mental health is and is not. Taking a position on cultural responses to mental health should be slightly comfortable because there is learning to do and change to be made in responses to that learning. The positions I take in critical mental health studies are not to dismantle medicine but to search for an evolution in the practical understanding of maintaining good cognitive, emotional and physical health which is needed.
Inevitably for anyone who claims an interest in mental health, there is a requirement to understand the sociology associated and to consider how to negotiate human rights issues as they play out in the lives of individuals and communities. Through becoming aware of the work which Tom Todd had been doing in relation to the Scottish Mental Health Law Review and helping coordinate a blog with academics in Australia around challenging corporate medical companies and their influence in medicine in their book ‘The illusion of evidence based medicine‘.
Tom Todd asked me to write an article for the blog on human rights which packs down all the research covered in this article to 800 words. I asked him if I could publish the long version and this is it. It includes annotations such as videos, papers and excerpts from original sources in the gray boxes so that the reader can make a more comprehensive examination of the arguments and sources. The intention here is to produce a study resource that allows readers to develop deeper insights into the issues raised by including the annotations.
Unpacking Human Rights in the British Context
When asked to write on this subject immediately what came to mind was what the worlds most quoted Human Rights scholar, Prof Philip Alstom, said about the UK: “…the advice I got clearly in the UK was don’t mention human rights…” (Alston, 2019).
This is the kind of backdrop we are working in as citizens of Britain, it may be counterintuitive for whom the culture works but there is something wrong in Eden. As Philip Alston continues, “…In other words, there’s been such a big campaign against it, such a backlash [19 minutes 58 seconds]….the theme that I’ve always pushed which is that poverty is a political choice…
…Poverty could be eliminated in virtually every country if the political elite actually wanted to do that, but they don’t, they consciously don’t. They want the money for themselves. And so looking at the US and the UK where you’ve got very wealthy economies, they had lots of choices but they still opt to have 15% or whatever of their population living in poverty so I thought it was very important to convey that message and document the linkage [23 min 28 sec]”.
(Transcript excerpt from the video ‘Do Human Rights Investigations Matter ? The Case of the UN Special Rapporteur on Extreme Poverty’, October 16, 2019 at NYU School of Law with Philip Alston, John Norton Pomeroy Professor of Law, Margaret Satterthwaite Professor of Clinical Law, and César Rodríguez-Garavito, Founding Director of Program on Global Justice and Human Rights – [19 min 58 sec to 23 min 28 sec])

Do Human Rights Investigations Matter ? The Case of the UN Special Rapporteur on Extreme Poverty’, October 16, 2019 at NYU School of Law with Philip Alston, John Norton Pomeroy Professor of Law, Margaret Satterthwaite Professor of Clinical Law, and César Rodríguez-Garavito, Founding Director of Program on Global Justice and Human Rights
I start this article touching on poverty because I argue in much of my work that poverty is the source of many harms which show up as mental and physical illness. Whilst there are frank and clear forms of poverty in certain parts of Britain, I argue that there are also new forms of poverty which culturally invisible because we collectively have not developed the common language to talk about them; without the words to articulate something people simply cannot discuss them.
We are presented the wealth of Britain as fact and in the shadow of these statements there are silences created. In many ways we are dealing with a brave new world where the anthropological histories have sublimed to new forms with claims they have shed their histories. Let me unpack that statement a little.
I am suggesting that whilst our current epoch states itself as having moved on from heritages of superstition and theocratic thinking of the past for science and enlightenment, those superstitions and forms of thought which were found in earlier times have reinvented themselves using the languages and rituals of modernity.
Poverties which existed as visceral and overt have shed their their old identities in a manner analogous to Jeremy Bentham’s Panopticon where the brutalities of the jailer were reinvented by the constant threat of surveillance. Bentham and the perspectives he laid out illustrated the move from prisoners being pilloried (public humiliation and physical abuse) to being “pilloried in the abstract” (made to wear masks and given a sense of being perpetually surveilled).
[page 6, Bentham J. (2011). The Panopticon Writings. Verso]
The prohibition on “cruel and unusual punishment” first appeared in the English Bill of Rights in 1689 and likely played a part in the rejection of Bentham’s Panopticon vision for prisons, hospitals, schools, sanatoriums, and asylums. In related ways I suggest that new means of impoverishment have been brought into existence along with the introductions of technology and lives encased in administrative systems, many of which lack transparency and are unaccountable – in part because the law has not evolved.
The way that concepts of seeming abstraction might have bearing in the visible world strikes me as yet to be fully grappled with and is a subtle notion which I am exploring. For example how privacy has a bearing on glucocorticoid (cortisol) stress levels and, in consequence, mental and physical health is impacted scarcely gets mentioned in relation to socio-economically poor communities being constantly surveilled by security cameras when correspondingly more wealthy neighbourhoods are not.
The effects which dysfunctional administrative systems have on health and wellbeing is another example of issues which involve an abstract nature which I suggest can significantly impact on mental and physical health – situations which can evoke the neurochemical cognitive blunting described famously by the work of Martin Seligman and Steven Maier in coining ‘Learned Helplessness‘. But, because the violence is sublimed into a structure where no individual person can be identified as inflicting a physical violence on a person or group, it is taken less seriously or doubted as to exist.
This work is research and writing I am doing as a part of problematising attitudes and approaches to psychological wellbeing, it is necessarily explorative in its nature searching for better perspectives that the ones which are operating today. As a part of Mad Studies it takes critical views as vital means to stimulating unsanitized, disruptive conversations needed to identify avenues of progress and also social justice issues.
As the context I live in and study is Britain, I pay special attention to the histories and anthropological structures which inform the context noting that human rights discourses are heavily disputed both in history and contemporary times. This I suggest has bearing on the common average person’s access to, and relationship with, protected areas of culture such as medicine and law.
Questioning the Closed Nature of Medicine
The furtive silences that fall around psychiatry and the discussion of medical privilege prompt the need to examine some of the factors which amalgamate in the confluence of the medical juncture. There is an Omertà operating in a sociological and physiological tangle which, if unraveled, threatens some of the regimes of truth which are rehearsed as modern absolutes structuring our cultural landscapes. There is a deep discomfort with openly discussing the privilege of power and position as it suggests an unsettling of the order which is seen in the status quo and gives comfort to so many as the devil we know.
Sometimes the relationships which people have with medicine are more related to narcissist/co-dependency models than to ones of dialogue and honest candour. The epoch we live in is shaped and derived from anthropologies and histories where straight jacket’s and surgical procedures were used to restrain people – ‘to quiet people down’. Our lot is to live through the chemical-industrial age, one where the prescription pad is the gateway to psychoactive drugs given out in the chemistry addled world, one where ipse dixit reasonings are dished out like candies.
Dissidence as Madness
Dare we critique the eminent professionals which have been placed in positions of authority and power; job roles which entice parents from particular socio-economic backgrounds to hothouse and push young minds to abandon other aspirations for ‘a respectable profession’ ? Dare we question the nature of madness or the impulses behind behaviours when standing out oft recreates one as a target, as a dissenter and trouble maker ?
I guess it is something of a madness to query power from the bottom, and dissent has historically been met in many places and times by assertions of power. It is for your own good it is often uttered; these are acceptable trade offs it is often said… Is it fair even to raise these points when the eminent professions are sacred for good reason ? The dynamics of this I am going to explore, so I argue yes, with the correct intent – one which is oriented around constructive remedy rather than an instinct for pugilism.
This very idea of questioning power has an important place in the history of madness. There is something of relativism going on in the use of the term mad. It is used to devalue the content of people at times, it is used to express uncontrolled emotion at others, and at other times it can be used to express elation at something out of the ordinary. Examining how simple labels can invalidate individuals who have had them applied is a part of the journey we must undertake if we are to get to a true and just understanding of mental health and mental illness.
If we look at the context of Russia, historically political dissidents were labelled with the psychiatric label of ‘sluggish schizophrenia‘. In his book ‘Punitive Medicine’ Alexander Podrabinek reveals to the reader the history of this label and the way which medicine has been used as an instrument of punishment (Podrabinek, 1980). As a medical assistant in the Soviet Union Podrabinek committed to paper how psychiatry was used for the suppression of political dissent before he himself was arrested and went into exile. He documents how psychiatry can be a place where civil liberties are absent and how ‘dissidents and socially dangerous individuals’ were interred in the identity of ‘sluggish schizophrenia’, as happened with the author Aleksandr Solzhenitsyn.
Podrabinek’s work illustrates how the psychiatric apparatus was complicit with the state wishes in Soviet Russia. This raises significant questions for other cultural contexts. We know, for example, that in America cultural dissidents such as civil rights protesters (Metzl, 2010) experienced psychiatry as a weapon revealing long and troubled ideological heritages that haunt the modern day.
“This book tells the story of how race gets written into the definition of mental illness. It uncovers the surprising ways anxieties about racial differences shape clinical encounters, even when the explicit races of doctors and patients are not at issue. The book also shows how historical concerns about racial protest reverberate through treatment institutions and subvert even well-intentioned efforts to diagnose people or to help them.
Ultimately, the book explores the processes through which American society equates race with insanity; and through which our definitions of both terms change as a result. It is well known, of course, that race and insanity share a long and troubled past. In the 1850s, American psychiatrists believed that African American slaves who ran away from their white masters did so because of a mental illness called drapetomania.
Medical journals of the era also described a condition called dysaesthesia aethiopis, a form of madness manifest by ‘rascality’ and “disrespect for the master’s property’ that was believed to be ‘cured’ by extensive whipping. Even at the turn of the twentieth century, leading academic psychiatrists shamefully claimed that ‘Negroes’ were ‘psychologically unfit’ for freedom.”
Metzl J. (2010). The Protest Psychosis : How Schizophrenia Became A Black Disease. Beacon Press.
However, when a political regime inters people, the power exercised can be easily be more easily identified (at least from the inside), but when such power is sublimed to the estate of the individual and family, power is not always so easily identified precisely because it is so close. Examples of the use of psychiatry as a weapon wielded in familial and community contexts are found in the histories of warehousing unmarried mothers (Robinson, 2016), ‘difficult’ family members (Wise, 2013), and gay people (Dickinson, 2016).
“Society assumed that marriage was the only acceptable way to bring up children, yet Maud considered marriage to be a symbol of subjection; she felt more strongly about this than about the risk of stigmatizing the children as bastards. She lied to them, in the cause of truth and independence for herself. Who are we to judge? Only her own family could – and did – do that. In some ways Maud’s decision may have been selfish, but it was made with conviction and integrity, and it worked for her.
From 1913 onwards, secrets like Maud’s and Fred’s might bring not only shame if they were revealed, but incarceration. That is when the Mental Deficiency Act was passed, with the euphemistic purpose of furthering and bettering provision ‘for the care of Feeble-Minded and other Mentally Defective Persons’. According to the Act, women could be deemed moral imbeciles as well as mental ones, and sent to an appropriate institution: a lunatic asylum. Moral imbeciles were defined as ‘persons who from an early age display some permanent mental defect coupled with strong vicious or criminal propensities’.
This chillingly included unmarried mothers who could not support themselves and were pregnant with their second (or later) child. Repeat offenders, in other words, whom the workhouses did not want to subsidize, or whose families had had enough of them. Under the terms of the Act, all it took for a moral imbecile to be committed if she was under twenty-one was a word from her parent or guardian. She did not even have to be medically diagnosed an imbecile. Her status as a young, abandoned and unmarried mother was enough. Those over twenty-one were in the treacherous hands of the Poor Law Guardians, who were often only too pleased to send them, with their babies, somewhere else.”
Robinson J. (2016), In The Family Way : Illegitimacy Between The Great War And The Swinging Sixties. Thorpe, Leicester, Chapter 1
“‘Oh yes, all those Victorian husbands getting their wives put away,’ said a good friend, when I told her my plans for a book about sane people being declared mad in the nineteenth century. Many others subsequently came out with something similar. But I hadn’t got very far into my initial archival dig when the variety of victims of malicious asylum incarceration became apparent; and it appeared that, anecdotally at least, this was slightly more likely to have been a problem for men than for women, certainly in the first sixty years of the century. As for those people who were indisputably mentally disordered, the mysterious lunatic in the attic was as likely to have been Bert as Bertha; the disturbed person in white in the moonlight on the Finchley Road would just as plausibly have been Andrew Catherick as Anne.
The following stories have been selected to highlight the range of people who had to fight for their liberty against the imputation of insanity. Presented roughly chronologically, the tales reveal the various definitions of madness put forward by the physicians, and the suggestions made by campaigners seeking reform of the asylum committal procedure. The stories bring to light, too, the protests that flared up periodically against the mad-doctors and the huge support shown for alleged victims of incarceration conspiracy.
What also emerges is a portrait of a bureaucracy – the Commissioners in Lunacy – that was failing to keep pace with both popular feeling and the views of the newspaper opinion-mongers. Above all, the ‘lunacy panics’ of the nineteenth century highlighted the fear that the English were sleepwalking into allowing the medical profession to curb individual freedom by labelling unconventional behaviour as a pathological condition, in need of cure or containment. ‘No rank in society is now exempt from the fear of being peculiar, the unwillingness to be, or to be thought, in any respect original,’ wrote John Stuart Mill, in On Liberty, published in 1859 – the year in which a series of notorious cases forced the government to appoint a Select Committee to probe the English lunacy laws.”
Wise S. (2013), Inconvenient People : Lunacy Liberty And The Mad-Doctors In Victorian England. Vintage Books, Preface
“On a winter evening in 1966, Percival Thatcher visited a public toilet on his way home from work in his family’s butcher’s shop in east London.1 Percival did not need to use the facilities in the public toilet; he was ‘looking for love’.2 Here an ‘exceptionally good looking young man’3 approached Percival and made a sexual advance towards him. When Percival responded to his advance, he was arrested – the young man was an undercover police officer. Percival was charged and subsequently convicted of importuning and conspiring to incite the police officer to ‘commit unnatural offences’.4
He was given the option of imprisonment or to be remanded provided he was willing to undergo psychological treatment to ‘cure’ his ‘condition’. In the belief that the psychological treatment would be a ‘better option’5 than imprisonment, he chose to receive the treatment. Percival was transferred to a local National Health Service (NHS) psychiatric hospital and was subjected to what he described as ‘a barbaric torture scene by the Gestapo in Nazi Germany trying to extract information from me’6 and he thought he ‘was going to die’.7
What Percival had agreed to was to undergo aversion therapy in a bid to cure him of his homosexuality. The behaviour of the police officer was not unusual and entrapment by undercover police officers during the 1950s and 1960s was common practice.8 Nurses were frequently involved in administering aversion therapies to cure such individuals of what were seen as their ‘sexual deviations’.9”
Dickinson T. (2016). ‘Curing Queers’ : Mental Nurses And Their Patients 1935-74. Manchester University Press
How do we disentangle the state from the individual and family or even community kinship relations ? Is it possible when the apparatus of the state is ultimately constructed and operated by individuals who inevitably come from a family nucleus and community relations ? What are the ideologies operating within the personal domain of the family nucleus and kith relations which are held as unquestionable much like the Soviet, American and British states demonstrated in their history ?
“The incarceration of free thinking healthy people in madhouses is spiritual murder, it is a variation of the gas chamber, even more cruel; the torture of the people being killed is more malicious and more prolonged. Like the gas chambers, these crimes will never be forgotten and those involved in them will be condemned for all time during their life and after their death.” – Aleksandr Solzhenitsyn, Quote in Punitive Medicine (Podrabinek, 1980)
Complicity: Scrutinising Rosemary Kennedy’s Story
Of course the problem is deeper, broader and more complex than is comfortable. Psychiatry speaks something of the views of society, its silences, its complicities, its fears of the unknown, the misunderstood, its malignancies… The power of a community to impose on people who do not ‘fit’ is a central axiom of group behaviour; this is discussed in relation to notions like absolute authority and social contract but also well detailed in the discipline of psychology. Pointed questions like ‘How many women have been medicalised – sectioned and/or drugged – for calling into question the bondage of marriage and the heritage of coverture ?’ are important to get beyond the inertia of deference to status quo.
What is done in the name of love and care is testimony to the capacity of human beings to be collectively ‘insane’ – a word which has its roots in ‘unhealthy’. What follows is an analysis of the early life of Rosemary Kennedy as a case study in complicity which reveals the horror possible through the power of psychiatric sanction. The sister of politician John F. Kennedy, her story illustrates how a series of unquestioned social realities ultimately gave rise to the lobotomisation of a young woman coming into the prime of her life.
When you read the biographies detailing what was known, it is apparent how the educational system, the institution of the family, the medical system, the church and government all participated in the effective destruction of this woman’s capacity to live an independent life. In short it is a high profile human rights travesty.
This human rights atrocity started in 1923 when Rosemary was five. She had been put in the Edward Devotion School kindergarten in Brookline where her teachers labelled her “intellectually disabled” and “deficient” due to her lagging behind her peers in the academic standards which were expected. This was how Rosemary was represented to her parents; she had been stated as a “retarded child”. Rosemary’s mother reportedly “did not like people who lagged behind or who were different” and had high aspirations for her.
[Chapter 3, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
It should be borne in mind how, at this time, the eugenics movement was in full swing. The Eugenics Record Office (ERO) founded by the renowned biologist, eugenicist and nazi sympathiser Charles B. Davenport was one of the leading organisers in the American Eugenics movement. It’s activities included collecting large archives of family pedigrees and sending field workers to analyze individuals at institutions like mental hospitals and orphanages across the US [“The Eugenics Record Office at Cold Spring Harbor Laboratory (1910-1939)”. The Embryo Project Encyclopedia. Retrieved 19.12.2022]. This was all bankrolled by the likes of the American financier and railroad executive E. H. Harriman, the Rockefeller Foundation and the Carnegie Institution. [Edwin Black (9 November 2003). “Eugenics and the Nazis – the California connection”. San Francisco Chronicle. Retrieved 19.12.2022]
To get a sense of how women and people were regarded in Massachusetts – the same state where Rosemary was in nursery school – at this time we can read a letter from the former lecturer in surgery at Harvard and senior surgeon at Boston City Hospital, George W. Gay who had been approached by the Massachusetts Commission for advice:
“The most feasible method of controlling women at present in this state is custodial supervision in an institution. Surgery offers an effectual preventative to conception, but it is not without some danger to life. With the male, however, there is a measure which is safe, practically painless, effective and free from any objections. Vasectomy … has been done a good many times with most satisfactory results to all concerned…. Your Commission is doubtless familiar with the admirable work which has been and is now being done by Dr. H. H. Goddard at Vineland, New Jersey….
Having spent a day there last year I became much interested in the results of his labors. They seemed to furnish undeniable evidence of the folly of allowing defectives to procreate. A large proportion of them are of no comfort or use to themselves or to society in general and moreover very many of them, as you well know, become public charges, for the support of whom you and I and everybody else who pays taxes have to foot the bills. This is all wrong and any experiment which is reasonable and practicable is worthy of trial.”
[collections.countway.harvard.edu/onview/exhibits/show/galtonschildren/eugenics-in-massachusetts]
Leading proponents of Eugenics including Charles Davenport, Henry H. Goddard, Harry H. Laughlin, and Madison Grant involved themselves in lobbying government for various ‘solutions’ to the problem of the ‘unfit’. Massachusetts had become a hotbed for this kind of thinking which we can see exemplified in this report on eugenic research from E. E. Southard, Harvard’s Bullard Professor of Neuropathology to the board of directors of the Eugenics Record Office in 1910:
“It is probable that Massachusetts is hardly surpassable in this country as a field for the study of eugenics, including under that name not only 1) eugenics proper, that is, the study of hereditary conditions tending to maintain society at par (the prevention of deterioration) but also 2) cacogenics, the study of hereditary forces tending to pull society down, as well as 3) the possibly Utopian variant, aristogenics, with its hope of elucidating the method by which the best stock is assembled and improved.”
[collections.countway.harvard.edu/onview/exhibits/show/galtonschildren/eugenics-in-massachusetts]
Rosemary Kennedy, for not coming up to one metric analysis or another, had been labelled mentally retarded by her teachers at the age of five in a state which had fully adopted eugenic ideologies. Her mother tried various social remedies to improve the academic performance of her daughter stating “one [child] may be smart in studies, one dull—one may be overconfident, another shy—and so a different approach must be made”. This was to shape the rest of her life affecting the way which Rosemary was treated by her parents, educational system, church and doctors.
[Chapter 3, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
The social pressures on the ambitious parents were high and the eugenic attitudes of the time and place meant that the attainment levels of the children reflected on them as public individuals and as a family embedded within a Catholic social structure. This resulted in the parents relentlessly seeking to ‘fix’ what they perceived in Rosemary as a pathology of under attainment.
As a Catholic family in the US they also had to negotiate the social pressures and prejudices the white anglo-saxon Protestant culture placed on them. For example, the father, Joe Senior had struggled to gain access to the social clubs which required certain invitations. This meant that they worked hard to try out anything on Rosemary which might change their daughter into the ‘high achiever’ they wanted. Here is an excerpt from Larson’s book ‘Rosemary: The Hidden Kennedy Daughter‘ which brings into relief the social atmosphere of the time:
“Rose’s consultations with a variety of doctors, psychologists, psychiatrists, academic specialists, and religious leaders took on a new urgency. None offered Rose what she thought was best for Rosemary, making her ‘terribly frustrated and heartbroken.’ Rose was accustomed to controlling her children’s social and intellectual lives, and she was determined that Rosemary would not be separated from the family. Joe Sr. believed, too, that keeping Rosemary at home or enrolled in nearby private schools provided her with more benefits than an institution for the mentally disabled would.
Both of them clearly understood that in the socially elite circles of Boston, New York, Europe, and elsewhere the pressure to institutionalize Rosemary, a choice many of their similarly situated wealthy counterparts made for their disabled children, would be great. Rose and Joe’s peers had been influenced by the powerful eugenics movement that swept Western societies during the latter part of the nineteenth and early twentieth centuries.
Eugenics was fueled by pseudoscientific claims that the human race consisted of ‘two classes, the eugenic and the cacogenic (or poorly born).’ The cacogenic, eugenicists claimed, “inherited bad germ plasm, and thus as a group . . . at the very least, should not breed.’ African Americans, immigrants, the poor, and criminals were often deemed cacogenics; fears of the ‘immigrant hordes’ streaming into American cities and the migration of African Americans out of the Deep South into northern and western cities led some native-born white Americans to embrace these beliefs.
The intellectually and physically disabled were another category of ‘defectives.’ Eugenics scientists and their followers believed that these individuals were also the products of inherited bad genes and should be treated much the same way as the mentally ill, criminals, and the chronically poor. Forced sterilization, they argued, was society’s cure. Some believed that spending money on insane asylums, poorhouses, and other charitable and social institutions and programs serving the mentally ill and disabled only encouraged the propagation of ‘bad seeds.’
The parents of ‘defectives’ carried these bad genes—an idea that placed the blame and shame squarely on families. Some of the most prominent industrialists, scientists, and political leaders of the late nineteenth and early twentieth centuries, including President Teddy Roosevelt, supported these views. Wealthy industrialists John D. Rockefeller, Andrew Carnegie, John Kellogg, Mary Williamson Harriman, and early feminist Victoria Woodhull became advocates of eugenics, funding spurious research promoting racial and ethnic discrimination through false claims of genetic deviance in nonwhite and ethnic minorities.
Labels such as ‘moron’ and ‘mental defective’ further complicated an already difficult life for Rosemary and her family. For Rose, reading eugenics literature and hearing such words describing her lovely daughter were stressful and heartbreaking. Christian beliefs and biblical tenets were no more helpful.
These overtly blamed parents for the physical, mental, and intellectual shortcomings and disabilities of their children, warning believers who failed to follow the Ten Commandments and the teachings of the Old Testament that God would punish them by ‘visiting the iniquity of the fathers upon the children unto the third and fourth generation.’ At that time the Roman Catholic Church routinely refused the sacraments of Holy Communion and Confirmation to intellectually disabled children, especially those with Down syndrome.”
[Chapter 3, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
“Rose [the mother] took her to ‘experts in mental deficiency,’ but their assessments and recommendations left Rose discouraged. The specialists told her that Rosemary had suffered from an unspecified ‘genetic accident,’ ‘uterine accident,’ ‘birth accident,’ and so forth.’ Some of Rosemary’s siblings believed that she also suffered from intermittent epileptic seizures. Eunice [the sister] remembered sudden and hurried calls to the doctor, who would rush to the house and administer injections and medications to Rosemary…
‘I can remember at the Cape the doctors coming in and giving her shots and then disappearing.’ Whenever one of these episodes occurred, the children were whisked away to another room or sent outside to wait until the doctor left, and only then were allowed to resume their activities. None of them dared ask what was wrong with Rosemary.
Gloria Swanson recalled Joe’s [the father] rage when she asked about Rosemary’s condition….They embarked on an illicit affair that lasted several years. Early in their liaison, Swanson overheard Joe talking on the phone with someone regarding the then ten-year-old Rosemary. He was ‘agitated’ and annoyed with the person on the other end of the line. Apparently, Joe was trying to get an unidentified doctor to treat Rosemary and ‘cure’ her. He offered to purchase a new ambulance for the hospital if the doctor would take Rosemary as a patient. The telephone call ended abruptly.
Swanson suggested that Joe bring Rosemary to meet with her personal physician in California, Dr. Henry G. Bieler. Bieler advocated a therapeutic diet as an alternative to drug therapies to cure a variety of illnesses. Swanson, like many other Hollywood stars, had followed his regimen and believed he held the key to lasting good health and mental well-being.
‘I had seen him [Joe] angry with other people, but now, for the first time, he directed his anger against me,’ Swanson wrote in her autobiography. ‘It was frightening. His blue eyes turned to ice and then to steel. He said they had taken Rosemary to the best specialists in the East. He didn’t want to hear about some three-dollar doctor in Pasadena who recommended zucchini and string beans for everything.’ Swanson persisted, encouraging him to consider Bieler. Joe reacted even more harshly: ‘I don’t want to hear about it! Do you understand me? Do you understand me?”
Drug Medications and Epilepsy
Before I go on to layer up the picture of the cultural context, I am going to first make explicit the physiological impacts which some of the drug medications would have had on the child Rosemary Kennedy. We can see that from an early age she was being exposed to ranging psychiatric drugs and treatments. The effects of early sedative medications like potassium bromide and barbiturates are well known. Kaculini, Tate-Looney, and Seifi (2021) give a history of anti-epileptic drugs and treatments which were popular in the context:
“At the turn of the 19th century, pharmacologic treatment of epilepsy began to gain traction. In 1912, Alfred Hauptmann discovered the anticonvulsant properties of phenobarbital, one of the most commonly prescribed medications for epilepsy worldwide today. Numerous Anti-Epileptic Drug’s were introduced in the following decades including ethosuximide, carbamazepine, valproate, and several benzodiazepines”
We can discover from scrutiny of standard pharmacological texts (such as the Rang and Dale and the British National Formulary), and drawing on fields such as toxicology, the liberal use of pharmaceuticals can create a range of problems which lead to iatrogenic harms through side effects that can get conflated with a prescribed psychiatric diagnosis. It does not take long to see that the list of drugs which have been used for epilepsy have wide ranging side effects including drowsiness, sedation, dizziness, lethargy, suicidal thoughts and behaviour etc.
Are teachers, clergy, parents, physicians and general society skilled enough in falsifiably distinguishing the effects of a drug from theorised conditions ? I would argue not particularly so when the drug gives rise to side effects which are attributed to the condition and where there are no scientifically detailed foundations for an organic basis of a condition against which checks can be made.
Excerpts from the Rang and Dale 8th Edition:
“Bromide was the first antiepileptic agent. Its propensity to induce sedation and other unwanted side effects has resulted in it being largely withdrawn from human medicine, although it is still approved for human use in some countries (e.g. Germany) and may have uses in childhood epilepsies.”
Carbamazepine
“Carbamazepine produces a variety of unwanted effects ranging from drowsiness, dizziness and ataxia to more severe mental and motor disturbances.4 It can also cause water retention (and hence hyponatraemia; Ch. 29) and a variety of gastrointestinal and cardiovascular side effects.”
Phenobarbital
“The main unwanted effect of phenobarbital is sedation, which often occurs at plasma concentrations within the therapeutic range for seizure control. This is a serious drawback, because the drug may have to be used for years on end. Some degree of tolerance to the sedative effect seems to occur, but objective tests of cognition and motor performance show impairment even during long-term treatment. Other unwanted effects that may occur with clinical dosage include megaloblastic anaemia (similar to that caused by phenytoin), mild hypersensitivity reactions and osteomalacia. Like other barbiturates, it must not be given to patients with porphyria (see Ch. 11). In overdose, phenobarbital depresses brain stem function, producing coma and respiratory and circulatory failure, as do all barbiturates.”
Ethosuximide
“Ethosuximide is well absorbed, and metabolised and excreted much like phenobarbital, with a plasma half-life of about 60 h. Its main side effects are nausea and anorexia, sometimes lethargy and dizziness, and it is said to precipitate tonic-clonic seizures in susceptible patients. Very rarely, it can cause severe hypersensitivity reactions.”
Phenytoin
“Side effects of phenytoin begin to appear at plasma concentrations exceeding 100pmol/l and may be severe above about 150|imol/l. The milder side effects include vertigo, ataxia, headache and nystagmus, but not sedation. At higher plasma concentrations, marked confusion with intellectual deterioration occurs; a paradoxical increase in seizure frequency is a particular trap for the unwary prescriber.”
Benzodiazepines
“Sedation is the main side effect of these compounds, and an added problem may be the withdrawal syndrome, which results in an exacerbation of seizures if the drug is stopped abruptly.”
Rang H. P. Dale M. M. Flower R. J. & Henderson G. (2016). Rang and dale’s pharmacology (Eighth). Elsevier Churchill Livingstone. Page 549 to 555
Excerpts from the British National Formulary 83rd Edition:
Phenobarbital (Page 364)
Agranulocytosis. anticonvulsant hypersensitivity syndrome. behaviour abnormal. bone disorders. bone fracture. cognitive impairment. confusion . depression. drowsiness. folate deficiency. hepatic disorders. memory loss. movement disorders. nystagmus. respiratory depression. severe cutaneous adverse reactions (SCARs). skin reactions. suicidal behaviours
With oral use: Anxiety. hallucination. hypotension. megaloblastic anaemia. thrombocytopenia
Sodium valproate (Page 357)
Common or very common: Abdominal pain. agitation. alopecia (regrowth may be curly). anaemia. behaviour abnormal. concentration impaired. confusion. deafness. diarrhoea. drowsiness. haemorrhage. hallucination. headache. hepatic disorders. hypersensitivity. hyponatraemia. memory loss. menstrual cycle irregularities. movement disorders. nail disorder. nausea. nystagmus. oral disorders. seizures. stupor. thrombocytopenia. tremor. urinary disorders. vomiting. weight increased
Uncommon: Androgenetic alopecia. angioedema. bone disorders. bone fracture. bone marrow disorders. coma. encephalopathy. hair changes. hypothermia. leucopenia. pancreatitis. paraesthesia. parkinsonism. peripheral oedema. pleural effusion. renal failure. SIADH. skin reactions. vasculitis. virilism
Rare or very rare: Agranulocytosis. cerebral atrophy. cognitive disorder. dementia. diplopia. gynaecomastia. hyperammonaemia. hypothyroidism. infertility male. learning disability. myelodysplastic syndrome. nephritis tubulointerstitial. obesity. polycystic ovaries. red blood cell abnormalities. rhabdomyolysis. severe cutaneous adverse reactions (SCARs). systemic lupus erythematosus (SLE). urine abnormalities
Carbamazepine (P.335)
Common or very common: Dizziness. drowsiness. dry mouth. eosinophilia. fatigue. fluid imbalance. gastrointestinal discomfort. headache. hyponatraemia. leucopenia. movement disorders. nausea. oedema. Skin reactions. thrombocytopenia. vision disorders. vomiting. weight increased
Uncommon: Constipation. diarrhoea. eye disorders. tic. tremor
Rare or very rare: Aggression. agranulocytosis. albuminuria. alopecia. anaemia. angioedema. anxiety. appetite decreased. arrhythmias. arthralgia. azotaemia. bone disorders. bone marrow disorders. cardiac conduction disorders. circulatory collapse. confusion. congestive heart failure. conjunctivitis. coronary artery disease aggravated. depression. dyspnoea. embolism and thrombosis. erythema nodosum. fever. folate deficiency. galactorrhoea. gynaecomastia. haematuria. haemolytic anaemia. hallucinations. hearing impairment. hepatic disorders. hirsutism. hyperacusia. hyperhidrosis. hypersensitivity. hypertension. hypogammaglobulinaemia. hypotension. lens opacity. leucocytosis. lymphadenopathy. meningitis aseptic. muscle complaints. muscle weakness. nephritis tubulointerstitial. nervous system disorder. neuroleptic malignant syndrome. oral disorders. pancreatitis. paraesthesia. paresis. peripheral neuropathy. photosensitivity reaction. pneumonia. pneumonitis. pseudolymphoma. psychosis. red blood cell abnormalities . renal impairment. severe cutaneous adverse reactions (SCARs). sexual dysfunction. speech impairment. spermatogenesis abnormal. syncope. systemic lupus erythematosus (SLE). taste altered. tinnitus. urinary disorders. vanishing bile duct syndrome. vasculitis
Frequency not known: Bone fracture. colitis. human herpesvirus 6 infection reactivation. memory loss. nail loss. suicidal behaviours
Phenytoin (Page 351)
Agranulocytosis. bone disorders. bone fracture. bone marrow disorders. cerebrovascular insufficiency. coarsening of the facial features. confusion. constipation. dizziness. drowsiness. Dupuytren’s contracture. dysarthria. eosinophilia. fever. gingival hyperplasia (maintain good oral hygiene). granulocytopenia. hair changes. headache. hepatic disorders. hypersensitivity. insomnia. joint disorders. leucopenia. lip swelling. lymphatic abnormalities. macrocytosis. megaloblastic anaemia. movement disorders. muscle twitching. nausea. neoplasms. nephritis tubulointerstitial. nervousness. nystagmus. paraesthesia. Peyronie’s disease. polyarteritis nodosa. pseudolymphoma. sensory peripheral polyneuropathy. severe cutaneous adverse reactions (SCARs). skin reactions. suicidal behaviours. systemic lupus erythematosus (SLE). taste altered. thrombocytopenia. tremor. vertigo. Vomiting
Ethosuximide (Page 339)
Aggression. agranulocytosis. appetite decreased. blood disorder. bone marrow disorders. concentration impaired. depression. diarrhoea. dizziness . drowsiness. erythema nodosum. fatigue. gastrointestinal discomfort. generalised tonic-clonic seizure. headache. hiccups. leucopenia. libido increased. lupus-like syndrome. mood altered. movement disorders. nausea. nephrotic syndrome. oral disorders. psychosis. rash. sleep disorders. Stevens-Johnson syndrome. suicidal behaviours. vaginal haemorrhage. vision disorders. vomiting. weight decreased
Committee J. F. (2022). BNF 83 (British National Formulary) March 2022 (83th ed.). Pharmaceutical Press.
When we see the fact that Rosemary had highly charged helicopter parents who set high societal social standards and drilled their children to their aspirations, it only takes the myopia of an educator to trigger a chain of events which proved disastrous for the child. In an education system which plays children off each other in a high stakes competition – i.e. the availability of future opportunities – someone at the age of five may not be equaling the same cognitive metrics which other children score on and so get labelled ‘slow’ or something more toxic.
A logic problem exists with prescription happy doctors dishing out drugs which have as side effects the symptoms they purport to cure. The pharmaceutical industry is quick to experiment on people and promote drugs which have wide ranging consequences; we need only look at the court records over the decades to know this. Add to this the mix of over the counter medicines infused with the heady advertising of miracle treatments invented in the laboratories of esteemed scientists carries with it considerable dangers which damage people.

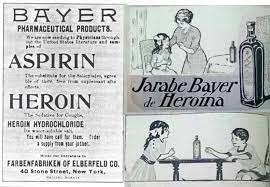
In the time Rosemary lived this a child might have been given any number of drugs which could have set the odds against them in any situation; as anyone who has tried sedatives might know, it is hard to function at your cognitive optimum when you are fighting the effects of drugs. Consider also that drugs such as heroine mixed with aspirin were being marketed and sold over the counter for children and adults for illnesses such as coughs and respiratory problems. You can see historical images illustrating this.
It is not unimaginable that Rosemary had a common childhood infection or minor ailment at some point in her young years and was medicated with a sedative medication which went on to impact her ‘academic performance’. It is also not unimaginable that she developed seizures from being given some sort of sedative medication due to the nature of many drugs producing profound biological shifts in state such as dependence, behavioural change and addiction/withdrawal symptoms.
This kind of iatrogenic feature of pharmaceuticals is not uncommon whereby the taking of one ‘medicine’ creates a different illness which is then subsequently medicated; but it is also not uncommon that medications which are given for a given symptom may also end up causing the given symptom – as illustrated in the case of some anti-epileptic medications.
Pharmacological Quagmire: The Sociology of the Medical Etiology
It is not enough to just look at the drugs to which this child was exposed but it is also important to construct a picture of how the medical world was constructing the etiology (causation or origination) of diagnoses alongside the cultural attitudes prevalent in the context. The cultural perception of seizures forged by the world of medicine had created pernicious and toxic images of people who suffered from seizures – many no doubt as a result of being exposed to some form of drug or another.
The work of Samuel-Auguste Tissot shaped medical discourse will into the last third of the nineteenth century. A reputed Calvinist Protestant neurologist, physician, professor and Vatican adviser, he had published ‘L’Onanisme: ou Dissertation Physique, sur les Maladies Produites par la Masturbation’ in 1764 which attributed epilepsy to masturbation.
[Lekka V. (2015). The neurological emergence of epilepsy : the national hospital for the paralysed and epileptic (1870-1895). Springer. Page 59]
“From this perspective, it should be noted that, during the first years under study, the methods of examination were, as one might have expected, rather embryonic, with the exception of the quite detailed categories ‘family history’ and ‘history’; in these two categories, the National Hospital’s doctors proceeded to the presentation and recording of even the minutest particulars of their epileptic patients’ personal life: from the their habits and their family tree to their potential proclivity to alcohol and the frequency of masturbation.”
[Lekka V. (2015). The neurological emergence of epilepsy : the national hospital for the paralysed and epileptic (1870-1895). Springer. Page 136]
It is well documented historically how the prevailing attitudes which dominated the ‘authority view’ of medicine prescribed to society how social and medical situations should be read. The notion of science had become a sort of totem by which values and attitudes could be projected on the world with impunity – a set of justifications which claimed to be objective and independent of the older vestiges of misapprehension, superstition and theocracy. The privileged culture of medicine was, and is, value laden whilst simultaneously denouncing, through an appeal to the ideal that scientific apprehension is free of such biases. Lekka details the kinds of social and cultural attitudes for us in the book ‘The Neurological Emergence of Epilepsy‘:
“Within the context of nineteenth-century hospital medicine, the practice of the persistent examination and measurement of the various bodily rates, the systematic observation, collection and recording of any kind of information, the constitution of the medical files, the strict definition of what constituted an anomaly and what a divergence from the ‘normal’, the pathologization of all ‘deviant’ states, the imposition of therapeutic/correctional/normative measures that aimed at the cure and, consequently, the generally accepted norm, constituted the regular beginning of every patient’s medical control and normalization.
Under these circumstances, a series of, until recently, putative ‘normal’ conditions of human life and, in a way, indifferent to power/knowledge networks, such as people’s birth, death, morbidity, disability, senility, even marital life, masturbation, mental health and childhood, all entered into the visual field of scientific medicine, being transformed into objects of medical research and intervention. At the same time, one of the most significant parameters of this procedure was health’s direct and obvious connection with what was considered as socially, politically, epistemologically and culturally ‘normal’, desirable and accepted.
Thus, it should not be considered as accidental the fact that medicine had primarily turned its attention to those social groups, which were generally considered as mostly threatening the social order and eurhythmy – among others, alcoholics, prostitutes, those suffering from venereal diseases, idiots, etc.; in other words, to those who were described as the ‘dangerous classes’. Without doubt, extremely indicative was the example of the so-called ‘mentally defectives’, to which epileptics were also included.
In late nineteenth century, within the frame of the general discussion on national degeneration and the emergent eugenic movement, mental deficiency emerged as a distinct medical, as well as social and political problem, marking the huge interest in both the human brain and the concept of the population. Everyone who was considered as a potential threat to the national prosperity and progress, was being rendered into an object of medical knowledge and, consequently, into the target of severe state intervention.
In this way, the category of the mentally defectives included a variety of people; beyond epileptics, it also included idiots, handicapped, deaf and blind persons, madmen, as well as criminals, alcoholics, those suffering from venereal diseases, etc. They were all treated as the result of the degeneration of their ancestors’ “pathological”, or even slightly “deviant”, condition. In this way, mentally defectives became gradually the archetypal representatives of the deterioration of the English race and the incarnated risk for its future.”
[Lekka V. (2015). The neurological emergence of epilepsy : the national hospital for the paralysed and epileptic (1870-1895). Springer. Page 156]
So we can see the attitudes which were likely projected onto the young Rosemary and how they also cast onto the Kennedy family in general. Whilst her father was fighting resistance to his inclusion in prestigious social clubs important for his political ambitions, the idea that one of his children was a mental defective would have been a weapon for others to use. We can see from the ‘History of Modern Epilepsy’ by Friedlander that the idea of sexual deviancy and its causing epilepsy had also been attributed to “parental masturbation”:
“W. Shanahan reviewed the status of this disorder in 1912, he noted that “research by means of the Wassermann test . . . [, discovered in 1906,] . . . into the part syphilis plays in epilepsy reveals the hereditary type as being present in a large percentage of cases developing in early life” [47]. Some other conditions which were supposed to predispose offspring to seizures were: changes in the nursing mother’s milk, due to excitement, anger [48] or worry [49]; parental masturbation [50]; puerperal convulsions [51]; and “traumatism” in a parent [4].”
[Friedlander W. J. (2001). The history of modern epilepsy : the beginning 1865-1914. Greenwood Press. Page 111]
“When a reason was offered about why excessive sexuality caused seizures, a frequent one was that it was irreligious and sinful. When a more physiological explanation was sought, a common one, using an 1892 quotation, was that there was an inordinate ‘expenditure of nerve force’ [203], or, as in a 1902 explanation, of ‘cerebral exhaustion’ [63].
Generally, masturbation was condemned more than excessive, but otherwise what was considered normal, sexual activity. Nothnagel, in 1877, made this point when he claimed that masturbation had a more marked effect on the nervous system than ‘excessive gratification of the sexual passion in the natural way’ [196]. Some relation between heredity and sexual activity’s epileptogenic nature was suggested by the idea that convulsions associated with an orgasm might be due to the inheritance of a ‘hypersensitive organization’ (‘nervous instability’ of Morel) [204].”
[Friedlander W. J. (2001). The history of modern epilepsy : the beginning 1865-1914. Greenwood Press. Page 124]
Add to all of this the fact that poor Rosemary was female, the notion of sexual agency in women was fraught taboo and therefore seizures may have resulted in a crucible of societal ills heaped on a young child which was to amount to the realisation of atrocities which befell her. We can start to construct how sociological cascades may be triggered on occasion which mount a series of societal projections on target individuals which sets the scene for moral disengagement and atrocity ? We can start to understand certain manifestations around and in psychiatry as social contagion.
“If only it were all so simple! If only there were evil people somewhere insidiously committing evil deeds, and it were necessary only to separate them from the rest of us and destroy them. But the line dividing good and evil cuts through the heart of every human being. And who is willing to destroy a piece of his own heart?” ― Aleksandr Solzhenitsyn, The Gulag Archipelago 1918–1956 (Solzhenit︠s︡yn, 2018)
Complicity and Coalescence: The Social Model
The benefit of the doubt is too commonly extended to those at the top of junctures of power relations and this leads to harms. That doctors could have reinforced the painting of Rosemary Kennedy as ‘intellectually disabled’ at such a young age should appall us. Not only this but that the medications which were heaped on her through her years were never queried for their impacts on cognition and wellbeing; this is a cultural horror show – one which I suggest lasts into this age.
To top this, that the vain drives of parents and educators are not questioned and are privileged over the health and happiness of an individual is an age old travesty shored up by industries of people who cater to the production of societies of exclusion and the damages which come of these. Such provocations are important if we are to get to the bottom of the disasters of medicalisation.
It seems that the intellectual capabilities of Rosemary were fine if we compare them with average capacities of today. Here is a letter which she wrote to her father illustrating the kind of cognitive work which she had been doing in a private school, this time in Brookline. Translating French into English is no simple task; and anyone keeping a journal and maintaining a range of communications with her family and others suggest how capable this girl was.
October 1, 1934
Darling Daddy,
J’ai beaucoup travaille a vous donner plaisir.
I have a travel book about Europe, and I am looking up and answering all the questions.
I have a French book, called, ‘que Fait Gaston?’ I am sending you a few lines from it.
The book is written all in French, and I have to translate it.
I am learning some History way back in the beginning when men lived in caves, and did not even know how to cook . . .
Did you receive my postcards and my letter? I am going to take some dancing lessons to get ready for the first Dance.
I hope soon to send you a letter in French. Give my love to all the family.
Rosemary
Whilst people can rationalise that Rosemary Kennedy experienced seizures and violent mood swings, it seems to me to imagine that mood swings might have been an entirely appropriate response to her environment; a patriarchal society riddled with prejudice which assumed all sorts of toxic ideas of people – and girls – who did not respond and fit into the plans dictated for them. Imagine being told that the seizures you are having are due to your unconfessed sexual proclivities ? Imagine how psychologically damaging being told this by your family and doctors would be. Being told as a child that you are mentally deficient, and yet witnessing the madness’ of the society which was telling you this – it is like a dark Franz Kafka story.
Shunted from school to school, from physician to physician, in a world which treated women (and many groups of people placed at disadvantages) perversely, in a high pressure family with social ambitions of political and economic climbing – what was this young woman to do ? What do all healthy young people do when perceiving they are yoked by other people’s ideas of who they want you to be ? I would suggest push back.
Tensions grew in her life and as a maturing young woman she expressed beauty. This brought with it considerable frictions within a family which already had a problematic relationship with sexuality, no doubt inflamed by the doctrine and culture of both the Catholic church and the prevailing Protestantism at large.
Her mother Rose held the perspective that sex should only be engaged with for the purposes of procreation. This was consonant with the conservative teachings of the Catholic church which Rose vocally cited. The role of sexuality in the sociological configuration we are examining that ultimately impacted so violently on Rosemary Kennedy is very significant. It shaped many outcomes. The following is an excerpt from Larson’s book which gives insight into how Rose Kennedy viewed the issue of sex for pleasure:
“It is not clear how early in the marriage Rose’s devotion to a very conservative version of Catholic womanhood became a barrier to sexual intimacy. The church deplored ‘deliberate cultivation of sexual union as an end in itself’ and upheld ‘the primary purpose[s] for which marriage exists—namely, the continuation of the race through the gift and heritage of children; the other is the paramount importance in married life of deliberate and thoughtful self-control.’
One of Rose’s friends from those years, Marie Green, later recalled that Joe found Rose’s refusal to engage in sex for pleasure extremely frustrating. Green reported that Joe often teased Rose about her confined and restricted view of sex. ‘This idea of yours that there is no romance outside of procreation is simply wrong,’
Marie heard Joe saying to Rose during one of their Friday-night get-togethers playing cards. ‘It was not part of our contract at the altar, the priest never said that and the books don’t argue that,’ Joe claimed. But Rose was resolute, and, in spite of what Joe argued and wanted, she had church teachings to support her. Green later recalled that after the birth of the Kennedys’ ninth child, Edward ‘Teddy’ Moore Kennedy, in 1932, Rose told Joe, ‘No more sex.'”
[Chapter 2, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
“When Kick turned thirteen, in 1933, Rose shipped her off to boarding school. ‘She was tremendously popular with the boys,’ Rose later wrote, ‘who were always telephoning her and asking her on dates . . . So boarding school was the answer, no phone calls or distractions from study, with girls her own age and whose families we all know.’ Keeping her girls under control was a significant priority. There is no explicit record of Rose’s thoughts on Rosemary’s sexual maturation. She had read the literature of the era, however, on female ‘defectives’—how they were more likely to become promiscuous, to have children with similar disorders or worse, and to create a more dangerous ‘class’ of criminals, prostitutes, and ‘feebleminded’ offspring.”
[Chapter 4, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
Here in the following excerpt, Larson discusses the likely candidate for the red pills which Rosemary had written about in her diary that she been prescribed and taking for years; the excerpt also touches on the troubled responses to the sexual maturation of this young woman:
“Though there is no way to tell what type of seizures Rosemary suffered from, any kind would have been frightening, exhausting, and debilitating. Treatment at the time would have included some form of sedative, like Luminal, the addictive barbiturate in red-pill form that Rosemary may have already been taking for years, to calm her after the worst of a seizure was over. In those days, however, treatment for epilepsy and nonepileptic seizures was limited and mostly ineffectual. Rosemary’s striking beauty—lovely features, a broad, perfect smile, and a buxom figure—continued to attract men’s attention. Rosemary had proudly told her father earlier that summer that even that ‘Saks man’ told her ‘he thinks [sic] I am the best looking of the Kennedys.’
In a household both highly sexualized on the male side and notably repressed on the female side, Rosemary’s beauty was a special threat. Lem Billings [friend of the father and family] suggested an additional diagnosis to journalist Burton Hersh: Rosemary was ‘sexually frustrated,’ a view surely more telling about Billings’s own sexual outlook than Rosemary’s, but his belief was rooted in common views about intellectually disabled and mentally ill women—attitudes shared and feared by Rosemary’s parents.
Twenty years after women had finally gained the right to vote, society’s lingering nineteenth-century ideas played heavily on social, religious, and scientific attempts to control women’s more public and expressive sexuality. This had devastating consequences for the country’s most vulnerable and weakest women, mentally ill and disabled women who faced victimization through forced sterilization and institutionalization at alarming rates. Interestingly, in spite of being effervescent, outgoing, and flirtatious, the slim-figured Kick was viewed as less sexually suggestive than Rosemary.
Though open and frank about sex in conversation, Kick [the sister Kathleen ‘Kick’ Kennedy] had no experience with intimate sexual contact, and her male friends knew that her religious background would preclude her from engaging in any sort of premarital sexual activity. In fact, Kick wished privately to her best friend, Charlotte McDonnell, as many of her friends were ‘pairing up’ and getting married, that she could remain single forever and go to parties, instead, every night. Yet no male contemporary of Kick’s ever described this party girl as ‘sexually frustrated,’ and it was Rosemary’s potential and physically obvious sexuality that her parents found dangerous.”
The mother attempted to regulate Rosemary’s life through sending her to a series of schools and summer camps ensuring that she was watched all the time. Rose and Joe Snr (the parents) turned to the Catholic Church however historically the church offered little help to families with children suffering from intellectual and physical disabilities. It was in 1917 through the development of Benedictine monk Thomas Verner Moore’s project of Saint Gertrude’s School of Arts and Crafts that this faith community started to open its thoughts to offering support.
Moore cultivated a “clear vision of what the Catholic Church needed to do for its mentally disabled members,” and aimed to bring together science and faith in clinical and social service oriented approaches. With proximity to the Catholic University and Trinity College it served to train nuns and laypersons in special education for those with disabilities.
There, a clinical care center was established at the university for mental illness and disabled children with significant funding coming from the Rockefeller Foundation in 1939 along with money from wealthy Catholic donors. It would be a major site for Catholic professionals to conduct research for “the treatment of emotional and behavior disorders” and psychiatry.
In 1940 Rosemary was placed at Saint Gertrude’s which by that time had fully integrated with the Child Center at the university. Culturally lauded as a therapeutic setting, Rosemary’s presence for public appearances had been described to function as a teacher’s aide. Unfortunately Rosemary did not find this move to be therapeutic, her mother writing later that “disquieting symptoms began to develop” and there being “noticeable regression…her customary good nature gave way increasingly to tension and irritability”. Larson describes this period in the following excerpt:
“Her outbursts of rage came on more frequently and unpredictably. Rose’s [the mother] niece Ann Gargan—the daughter of Rose’s sister Agnes—later revealed that Rosemary had become incorrigible at Saint Gertrude’s. She defied the nuns, the staff, and their rules. ‘Many nights,’ Gargan told historian Doris Kearns Goodwin, ‘the school would call to say she was missing, only to find her out walking around the streets at 2 a.m.’ The nuns would bring her back, clean her up, and put her to bed. Her explanations about where she had been or what she had been doing made no sense, or else they made frightening sense.
‘Can you imagine what it must have been like,’ Gargan recalled, ‘to know your daughter was walking the streets in the darkness of the night, the perfect prey for an unsuspecting male?’. Joe Sr. expected his children to keep ‘out of the [newspaper] columns,’ granddaughter Amanda Smith recalled. His fears that Rosemary would end up as fodder for gossip columnists profoundly informed his and Rose’s efforts to keep her sequestered. What happened to Rosemary during that time has remained a mysterious and complicated story, with a thin trail of evidence and mostly conjectured interpretation.
Even family members remain mostly in the dark about what truly happened to Rosemary during her time at Saint Gertrude’s. Rosemary remained at Saint Gertrude’s through 1941. Joe, no longer ambassador but living in Palm Beach playing golf and keeping up with news of the war in Europe, had looked into having Rosemary attend Wyonegonic Camp in Denmark, Maine, during the summer of 1941, but there is no record of Rosemary having attended.”
[Chapter 7, Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.]
Kennedy family chronicler Laurence Leamer wrote about Teddy Kennedy’s memories of Rosemary’s disposition and contrastingly moots the fears which she evoked in her parents:
“Teddy knew nothing of the difficulties his big sister was facing. He only knew that good Rosemary was his gentle friend. She was not rushing out on dates or off with her friends like his other big sisters. She was there, ready to talk to him and play. To him, she was a dream of what an older sister should be. ‘I just had the feeling of a sweet older sister … who was enormously cheerful, affectionate, loving perhaps even more so than some of the older ones,’ Teddy reflected. ‘She always seemed to have more time, and was always more available.’
Rosemary could have handled a menial job, but in 1941 there was no place for her to go. In recent months, she had begun to suffer from terrible mood swings. She had uncontrollable outbursts, her arms flailing and her voice rising to a pitch of anger. In the convent school in Washington the nuns were having a difficult time managing her. She sneaked out at night and returned in the early morning hours, her clothes bedraggled. The nuns feared that she was picking up men and might become pregnant or diseased.”
[Chaper 10, Leamer L. (2002). The Kennedy Men: 1901-1963 : The Laws of the Father (1st Perennial). Perennial.]
The family hysteria about public appearances and control over the activities of the first born daughter manifested especially around the sexuality of Rosemary. These deep fears are cited in Doris Kearns Goodwin’s book ‘The Fitzgeralds and the Kennedys‘:
“Something had to be done, not only for Rosemary but for her mother, who could not rid herself of the fear that something terrible was going to happen to her daughter. ‘I was always worried,’ Rose later noted, ‘that she would run away from home someday or that she would go off with someone who would flatter her or kidnap her, as the kidnapping craze was on then.’ And beyond these concerns, there was the deeper fear that Rosemary would get pregnant. At twenty-one she stood five feet seven inches tall, with a full rounded figure, a clear complexion and excellent features. ‘She was the most beautiful of all the Kennedys,’ Ann Gargan recalls. “
[Goodwin, D. K, (1987) The Fitzgeralds and the Kennedys, Simon and Schuster, Page 640]
Rosemary’s life had become a series of placements to be overseen by her parents and people in their employ. Studiously managed by her mother Rose and the Rolodex she kept on all details of her children’s life events, one cannot help but wonder how much aspirations and fears had eclipsed the real Rosemary in the thoughts and actions of her parents. Drawing again on ‘Rosemary: The Hidden Kennedy Daughter’ we find an insight into the micromanaged conditions she was living under:
“Through family acquaintances, Rose found what she believed to be a positive placement, Camp Fernwood, in western Massachusetts. She approached its owners and directors, Grace and Caroline Sullivan, to discuss Rosemary. The two women were the daughters of Michael Henry Sullivan, an attorney and former chairman of the Boston School Committee. In 1909, he had become the youngest judge ever appointed to the bench in Massachusetts. Located along the shores of Plunkett Lake, in Hinsdale, Camp Fernwood was a Catholic summer sleepaway camp for girls ages six to sixteen.
Rosemary seemed excited about attending the camp and about what she might be doing there during the summer. She believed, and no doubt was told, that she would be a ‘junior counselor,’ teaching youngsters as she had done in England. ‘But isn’t it interesting,’ she wrote her father in London on the Fourth of July after arriving at the camp, ‘but [sic] me being a junior counsellor the first year. They thought I had experience [sic] in Arts, and Crafts in Europe. So, I am teaching it now. I have the younger girls. And another girl Alice Hill, as the bigger girl in Arts, and Crafts. So, the two of us run it.’
Rose should have given the Sullivan sisters some indication that Rosemary, an adult woman, was intellectually disabled, but it seems she did not share much with them—certainly not that the staff would need to monitor Rosemary every day to be sure she rested, ate properly, completed her tasks, and remained composed with the children; or that they would be called to calm her rages, to constantly reassure and compliment her, and to monitor her every move.
Whereas Kennedy family lore long perpetuated the myth that Rosemary was hired to be a counselor at the camp, Sullivan family records reveal a different story. In the spring of 1940, while Rosemary was still living in England and the Sullivan sisters met Rose in New York to discuss Rosemary’s placement, they were completely unaware of the extent of her disabilities. All they knew was that Rose was hoping her twenty-two-year-old daughter—who had received Montessori training in England to become a teacher’s assistant—could find a spot for the summer at the camp.
She would require, Rose told them, a special counselor to accompany her at all times. Rose did not explain fully why this was so necessary. Terry Marotta, Caroline Sullivan’s daughter, wrote that her mother later recalled that ‘she should have known the minute Mrs. Kennedy arrived [in New York] without her daughter that the girl was not as ‘able’ as Rose was leading them to believe.’ To Rose’s relief, the Sullivans accepted Rosemary into the camp program—not officially as a paid junior counselor, but rather as a camper who needed guidance herself.
In a July 1 letter from Rose’s secretary and the younger children’s governess, Elizabeth Dunn, to the Sullivan sisters, Dunn conveyed Rose’s requirement that the camp staff be ‘sure her [Rosemary’s] arch supporters are in her shoes correctly’ and that Rosemary sit at the ‘diet table if you can encourage her to.’ Additionally, Rosemary should ‘use Arts and Crafts Shop as much as possible. Have tennis lessons as often as practical,’ and ‘do exercises for her arches.’
These ‘very important’ instructions were the ones Rose chose to convey—not suggestions on how to handle an adult woman prone to anger, or likely to be ‘fierce’ with the children, or anxious about changes in her daily routine and environment. Clearly, in spite of her instructions concerning Rosemary, Rose gave little thought to the campers or to the abilities of Fernwood’s staff to cope with Rosemary. There were problems from the start.
One family friend later recalled that the Fernwood staff did not realize that Rosemary’s shoes were ill fitting until they noticed her feet bleeding. Frustrated, the Sullivan sisters took Rosemary to their own podiatrist in nearby Pittsfield, Massachusetts, to help relieve her intense discomfort. Rosemary may have consciously followed her mother’s instructions about putting on a positive public face and not complaining, but in this case she was clearly carrying the mandate to the extreme.
The sisters were shocked when they discovered that Rosemary did not properly dispose of her stained sanitary napkins but rather stored them in her camp trunk. They were deeply worried by Rosemary’s habit of wandering off. Caroline Sullivan, whom Rosemary called ‘Cow’ because she could not pronounce Caroline’s nickname, ‘Cal,’ eventually had Rosemary sleep in her private quarters, with a bed placed up against the door to prevent her from wandering off in the middle of the night. After three weeks, the Sullivans had had enough, and they requested that Rose come and take Rosemary home. Rose told them she could not come to the camp and that it was up to them to get Rosemary to New York”
Larson K. C. (2016), Chapter 6, Rosemary: The Hidden Kennedy Daughter, Mariner Books / Houghton Mifflin Harcourt.
In this short verbatim excerpt I want to pick up on a few points in order to surface the concerns which are relevant to critical readings of the sociology. We can see dueling narratives at play about why Rosemary was going to the camp which the Sullivans ran. Rose, the mother, had created a veritable prison where all of Rosemary’s activity was overseen. The narrative with those whom Rosemary had been placed with was obviously different from the version which she herself encountered.
Believing that she was to be doing meaningful activity as a junior counselor practicing her skills, she had in fact been placed as a ward with people who were closely associated with the parents; this likely meant some level of extra communication between the Sullivans and the parents from which Rosemary was divorced. We can imagine emotional cataclysm which might be involved when Rosemary discovered that she was not going to exercise her Montessori teaching but was there as a subject.
Larson as a writer leans towards accounting for mental disability without sufficiently scrutinising the sociological configuration which should inform our understandings of Rosemary’s lived experience. The power of psychiatric labels as social contagion is vast. In the majority of accounts expressions of emotion and anger have been medicalised and put down to esoteric illness rather than the terrible circumstances Rosemary found herself in. There is no questioning of the fact that the people around her might have been treating her badly. We can see Larson reinforcing the implicit assumptions of the psychiatric lens in her pointing out that Rosemary was “intellectually disabled” even though it had not occurred to the Sullivan sisters without it being expressly communicated by Rose Kennedy.
There could be read here information that suggests that the mother-daughter relationship had significantly atrophied or been absent due to the details such as Rosemary’s ill-fitting shoes or management of menstruation. It is not uncommon for young women to be culturally pressured into damaging aesthetics; the association of femininity with petit feet has a long and tortured history existing from foot binding to the present day where women get ‘Cinderella Surgery’ to reduce and reshape their feet.
Why Rosemary had such small shoes should raise questions about the relationship with the mother Rose; complex questions, questions which interrogate the culture and values as well as whether healthy communication was happening at all. Culturally Rosemary was exposed to a toxic mix of gendered values, some of which might have made her feel that her value was considerably rooted in society’s appraisal of her beauty as a woman.
We can certainly see clues as to the mother’s pressure to conform to certain aesthetics as indicated by her instructions to the Sullivans to steer Rosemary towards “the diet table”. As well as this we can clearly see that Rose Kennedy was in some way aware of Rosemary’s feet through her instructions to the Sullivans to make “sure her [Rosemary’s] arch supporters are in her shoes correctly” and remind Rosemary to “do exercises for her arches”.
A strong indicator of a breakdown of the mother-daughter relationship was the fact that Rosemary had taken to storing her used sanitary products in her camp trunk. The societal taboos around menstruation have long been a damaging influence on the lives of women. Again, in light of this we need to ask complex and nuanced questions about what is going on in the mother-daughter relationship sufficient for the daughter to have resorted to this. Was there any discussion about menstruation as a natural process and the management of periods ?
To be surveilled all the time by “a special counselor to accompany her at all times” to “monitor her every move” is something of a social trauma for anyone which would make any individual crave space to be alone. Her habit of wandering off is likely an everyday reality of any human, but when placed under constant guard it seems that taking a walk at night might be a perfectly normal activity. To disallow this and take total control over this woman in her twenties by barricading her in the same room illustrates to this writer a break down in normal civil arrangements.
This leads me onto the final weak point of analysis of this text with the focus on Caroline Sullivan, whom (it is reported) Rosemary called ‘Cow’ because she could not pronounce Caroline’s nickname, ‘Cal,’. I wonder as a reader whether this might have been a manifestation of Rosemary’s subtle push back at the domination of her every move. Under such circumstances it seems like any amusement might be life bread for Rosemary once she realised she was under the total control of these women. There is certainly no mention of speech anomalies prior to lobotomy in Larson’s book or other biographies.
This could have been a result of multimodal perception in that, once the relationship between Caroline and Rosemary had broken down the McGurk Effect played out the cognitive bias of Sullivan. Could it be possible that Caroline was hearing ‘Cow’ because she was feeling usurped by Rosemary’s failure to coalesce in the deference she expected ? Whatever happened in this juncture we know that Rosemary existed at the bottom of the juncture of power relations and that three weeks after her arriving Rosemary was to leave under imperfect circumstances.

Lobotomy: The Mutilation of Rosemary’s Brain
At the age of 23 it is reported that her father sanctioned a lobotomy in order to pacify her mood swings and make her more compliant. He was threatened by the idea that scandal would affect his political career and those career’s he had planned for his sons. The idea that they would not be known as ‘good Catholics’ was overwhelming for him:
“In 1941, unbeknownst to his wife and family, Joe Kennedy took Rosemary to be examined by Dr. Walter Freeman, a neurologist and psychiatrist who was also a professor at George Washington University. Joe had read about the doctor’s successes in Life, Time, and Newsweek magazines. Dr. Freeman’s diagnosis of Rosemary was ‘agitated depression.’ He claimed a lobotomy would not only relieve her of the rages she suffered but also render her happy and content. The prestigious doctor, an imposing six feet tall, bore a professorial-looking mustache and beard. He assured Joe that a lobotomy was the best option available for Rosemary.”
[Chapter: Rosemary’s Surgery, Koehler- Pentacoff E. (2016). The Missing Kennedy: Rosemary Kennedy and the Secret Bonds of Four Women. Bancroft Press.]
The following is an excerpt from Ronald Kessler’s ‘The Sins of the Father; Joseph P. Kennedy and the Dynasty he Founded‘ which takes us through one of the surgical barbarisms which the medical world was meting out on large populations. It is not only an account of the deliberate incapacitation of the brain of Rosemary Kennedy in order to control a young woman, but it is also an indictment against the inordinate and unquestioned powers the medical world has in fulfilling dubious wishes of the agency laden individuals:
“The lobotomy era had begun in the early 1930s when a pair of neurological scientists severed the frontal lobes of chimpanzees’ brains, rendering them docile and relaxed. They presented their findings to a conference in London in 1935, where Portuguese scientist Egas Moniz decided that what seemed to work for apes might work for humans. He returned to Lisbon and drilled holes in the skulls of twenty hopelessly ill mental patients. He reported that most of them ‘recovered’ or ‘improved.’
Dr. Walter J. Freeman, who had an appointment to St. Elizabeths Hospital in Washington and was a professor of neurology at George Washington University School of Medicine, read his reports and became an evangelist for the procedure. As a partner, he enlisted his associate, Dr. James W. Watts. In 1935, Freeman had invited Dr. Watts to join the neurology department. Born in Lynchburg, Virginia, Watts had obtained a medical degree from the University of Virginia and received training in neurosurgery at Massachusetts General Hospital in Boston. He eventually became chief of neurosurgery at George Washington University Hospital.
He was also a consultant in neurological surgery at St. Elizabeths Hospital, Washington’s city-owned mental hospital. Highly regarded in medical circles, Dr. Watts became the ninety-first president of the Medical Society of the District of Columbia. Both doctors sincerely believed in what they were doing. At the time, no drugs were available to treat mental illness. Those with severe symptoms were confined to mental hospitals, often for the rest of their lives.
As described in a published paper by Drs. Freeman and Watts, lobotomies relieved ‘certain patients of mental symptoms by a destructive operation carried out upon their frontal lobes,’ which are responsible for the brain’s higher intellectual functions. The operation entailed ‘cutting the matter of each frontal lobe.’ The doctors claimed that the procedure ‘bleaches the affective component connected with the consciousness of the self’ in those ‘whose preoccupation is fixed and unyielding….’ This ‘allows the personality to appear in purer form,’ with only minor changes in ‘energy and intelligence.’
Evaluating their own work, the doctors rated the results ‘good’ in more than half the cases. Their article showed pictures of people who looked depressed before the operations; afterward, they appeared to be smiling but were glassy-eyed. The doctors admitted that some patients ‘remain somewhat indolent, lacking in the imaginative capacity to see for themselves what needs doing. ‘At least three patients died on the operating table. Yet they said others were freed from ‘the restraints imposed by timidity, sensitiveness, or embarrassment.’
In fact, in most cases, the operations substituted one set of disturbing symptoms for another. Instead of being disruptive and irrational, the patients essentially became zombies because of brain damage. At the time Joe asked the doctors for their help, they had performed only sixty-six prefrontal lobotomies, nearly all the lobotomies performed at that time. While Dr. Freeman supervised, Dr. Watts did the surgery. In the only interview he ever gave on the subject, Dr. Watts described to the author how he performed the lobotomy in the fall of 1941.
After Rosemary was mildly sedated, ‘We went through the top of the head,’ Dr. Watts recalled. ‘I think she was awake. She had a mild tranquilizer. I made a surgical incision in the brain through the skull. It was near the front. It was on both sides. We just made a small incision, no more than an inch.’ The instrument Dr. Watts used looked like a butter knife. He swung it up and down to cut brain tissue. ‘We put an instrument inside,’ he said. As Dr. Watts cut, Dr. Freeman asked Rosemary questions. For example, he would ask her to recite the Lord’s Prayer or sing ‘God Bless America’ or count backward.
Her pulse became more rapid, and her blood pressure rose. ‘We made an estimate on how far to cut based on how she responded,’ Dr. Watts said. When she began to become incoherent, they stopped. ‘I would make the incisions, and Dr. Freeman would estimate how much to cut as she talked. He talked to her. He would say that’s enough.’ Beginning in 1946, Freeman and Watts refined their methods. Instead of cutting holes in patients’ skulls, they inserted a device that looked like an ice pick through the eye cavity.
Freeman, who has since died, later estimated that between 1936 and the late 1950s, he performed or supervised four thousand of the forty thousand to fifty thousand lobotomies performed in the United States. By the late 1950s, the lobotomy era had ended. Tranquilizers replaced the procedure. Dr. Watts told the author that, in his opinion, Rosemary had suffered not from mental retardation but rather from a form of depression. At the age of ninety, he could not recall with certainty what kind of depression she had. Then as now, the terminology of psychiatric illness was constantly changing.”
[Chapter 16, Ronald Kessler – The Sins of the Father_ Joseph P. Kennedy and the Dynasty He Founded-Grand Central Publishing (2012)]
Questioning the Label that Plagued Rosemary
Gerald O’Brien is a professor in the Social Work Department at Southern Illinois University Edwardsville. Primary research interests are historical issues in disabilities, analysis of the Americans with Disabilities Act, and contemporary ethical issues that pertain to persons with disabilities. He has studied the life of Rosemary Kennedy and written on her role in the family saying “Rosemary’s presence within the Kennedy home may have been a much more important component of the family’ rise to prominence than most scholars appear to believe.”
[O’Brien, G. (2004). Rosemary Kennedy: the Importance of a Historical Footnote. Journal of Family History, 29(3), 225–236. doi:10.1177/0363199004266849]
Gerald O’Brien is quoted in an article published in The Independent newspaper as saying about Rosemary Kennedy: “I am not convinced that she was mentally disabled. Back then, mental retardation was not a clear category and it wasn’t gauged in any accurate way.”
[El-Hai, J. (2005), The Exiled Kennedy. The Independent. Retrieved 29.12.22]
This has been the story of Rosemary Kennedy used to demonstrate the complicity, culpability and perversity possible in social configurations which link family, church, medicine, community, gender, age and state in detrimental sociological cascades. I suggest that such cascades still occur in in psychiatric contexts but they are dressed with different garb. The surgical blades may have been replaced with chemicals, the language and diagnoses may have morphed into a new set of unproblematised idioms, the social construction of disadvantage may have changed in its structure, but I suggest the uncomfortable truth that such issues are still live in our societies today.
Old wine in new bottles, for many a vanity of the modern is to imagine all the problems of the past have gone with the turning of a calendar page and the newness of a haircut. The comforting idea is to imagine that progress is linear and ever in the vein of improvement; this fronts the egotism of the now whilst simultaneously the habitual is reconstructed in ritual structures that get lauded as tradition and heritage. There is no doubt that sometimes humans want to drink the coolaid rather than reassess the appropriateness of the people and ideas we have placed our faith in.
The Medical Alienation of Human Rights
The psychiatric juncture is a place of extraordinary alienation; for us to understand fully the state of the relations of the medical institution to the people we must first apprehend the political philosophies which contend to account for authority. Britain is a culture which has historically resisted the notion that people have inalienable rights equal to every other (Tully & Skinner, 2009). In Britain the dominating culture has been informed by political philosopher Thomas Hobbes where he articulates in the work ‘Leviathan‘ how the rights of people are alienated from the individual to some person who has been suggested as an ‘absolute sovereign’ stated as infallible and unquestionable.
The work Leviathan lays out various axioms including restricting freedom of speech for censorship by a governing hierarchy. It expresses a tacit social contract whereby, even unawares, people have given up their rights to an absolute sovereign so that they may have decisions made for them and ruled over in order to preserve what they notionalise as ‘the commonwealth’. This part of political theory is important as the privilege of landed gentry and a historical scheme of monarchy has shaped who is allowed to practice in protected professions such as medicine and law. A key legal moment of this is laid out in the Elizabethan Statute of Artificers.
In response to this a countervailing political philosophy was laid out by the thinker John Locke in his 1689 Second Treatise of Civil Government. In this ground breaking work he detailed that ‘freedom from absolute, arbitrary power is so necessary to, and closely joined with preservation that they cannot part with it…a person… cannot by compact or consent enslave their self to any one nor put their self under the absolute arbitrary power of another’. This basic idea expressed the political foundations of human rights which are inalienable – meaning that they cannot be removed – from the individual even should the person will it.
[Locke, J. (1955). Of civil government: Second treatise. Chicago: Henry Regnery Co. Chapter IV]
Tully & Skinner in their book ‘Approach To Political Philosophy‘ flesh out and develop variations on this idea which the reader can see in the excerpt given below. Law can be understood as a part of a social system which reflects and makes inflections on the collective, and ultimately the individual behavioural level. Societies of peoples are socially constructed and the ideas prominent in the landscape commonly reach prominence in the thoughts and actions of individuals.
Thus for us to understand medicine and psychiatry properly in their realised forms we must be willing to look at insinuating systems such as law and economy (etc) as these impart dynamics on the construction and replication of systems. In short a legacy policy system will shape how people do things in a given context and the material outcomes which come of the policy systems.
“The fourth step in the juridical problematic is the way in which political power is placed in the hands of monarchs and/or representative bodies. It is a historical, logical and normative question concerning the rights and conditions under which the great centralizing monarchies or the representative institutions of early modern Europe exercised political power. In the natural freedom tradition two general genealogies were proposed.
The first and dominant explanation, which Locke adopted in the Two tracts, is that the people as a corporate whole, and usually acting through their representative body, consent to alienate completely political power to the monarch and to renounce the right of self-defence. The monarch is sovereign, above the law and therefore absolute. The monarch is said to be bound by natural law but, since the people have renounced their right to defend themselves, only god can punish the ruler’s transgressions. Most absolutists mitigate this doctrine of non-resistance in cases where the monarch alienates his kingdom or sets about destroying his subjects. Then, as William Barclay puts it, and Locke quotes with approval, the people may defend itself (without injuring the king), usually through its representative body. Or, as Grotius and Pufendorf concede, an individual may defend himself against direct attack by a murderous tyrant.
The main argument for alienation in its pure or mitigated form is that if sovereignty is shared by monarch and parliament (or estates), or if the people do not renounce their (or its) right to judge when it is a situation of self-defence, then, given human partiality, this will lead to disagreement, dissension, tumults, and so to civil war. The idea that political power is shared by parliament and monarch was castigated as a throwback to the strife-ridden feudal past and an impediment to centralization and modernization under absolute monarchy.[59]
The second argument, famously advanced by Rousseau against the Two Treatises, is that unless alienation is complete no sovereign is formed and people remain in a quasi state of nature.[60] Locke used both of these arguments in the Two tracts. The second genealogy is that the people, as a whole, consent or contract to conditionally entrust political power to the monarch or to monarch and parliament (in mixed monarchy theories), or to parliament (in parliamentary sovereignty).[61] When the ruler abuses the trust it is broken and power devolves back to the people. Then, the people may defend themselves either through parliament or, if it is a mixed monarchy, through a natural representative body such as Lawson’s forty courts of the forty counties. As we have seen no one was willing to say that dissolution of the trust returned the exercise of political power to the people either individually or collectively.
In the Two treatises Locke adopts the trust theory of the relation between government and governors and adapts it to his individual account of political power. There are three reasons why he accepted the trust hypothesis. First, according to the alienation hypothesis, the sovereign is by definition outside of political society, since he is not subject to law, and thus absolutism is not a form of political society (2.90). Further, since the people resign their right to judge and punish him for violations of natural law, it is worse than the inconveniences of the state of nature since they have no right to protect themselves against his violence. Hence it would be irrational to consent to alienate: ‘to think that men are so foolish that they take care to avoid what Mischiefs may be done them by Pole-Cats or Foxes [in the state of nature], but are content, nay think it safety, to be devoured by Lions [in absolute monarchy]’ (2.93). This is clearly directed against any natural freedom theory of alienation, whether Grotius, Hobbes, Pufendorf, or Locke himself in the Two tracts. Not only is it irrational. Since it involves transferring absolute power over one’s life to another, it presupposes that individuals have the right to dispose of their own life. Locke points out to his Christian audience that only god has such a right (2.23, 2.135, 2.149, 2 I7L 2.222). ”
Tully, J., & Skinner, Q. (2009). Approach To Political Philosophy. Cambridge, Gbr, Cambridge University Press. Http://Public.Ebookcentral.Proquest.Com/Choice/Publicfullrecord.Aspx?P=4638354. P 29
The notion of universal and inalienable human rights is not one which belongs particularly to western conception of social configurations. We can see that documents of human rights long predate the work of John Locke which hail from origins of ancient Near East, Mesopotamia and of Jewish diaspora. For example, the Cyrus Cylinder of Cyrus the Great has been suggested as the earliest declaration of human rights dating to 6th century BCE; it has also been suggested by scholars that rulers in ancient Iraq had been making comparable declarations for two millennia before the time of Cyrus.
[Neil MacGregor, “The whole world in our hands”, in Art and Cultural Heritage: Law, Policy, and Practice, pp. 384, ed. Barbara T. Hoffman. Cambridge University Press, 2006. ISBN 0-521-85764-3]
Whilst I am speaking to my context I also make a keen effort to illustrate how the notion of human rights are not unique to the anglicised world or one particular place and time. For the purposes of the context here my interests are to draw a focus on the Lockean line of thinking as originally being penned in England and shaping British, and ultimately Common Law in the English speaking world.
Britain, Medicine and Human Rights
In this section I am going to explore the British relationship with human rights relating this to the medical psychiatric context. I am also going to relate how finance and corporate structures represent governance systems detailing how the heritage of absolute authority shapes the practice and discourse of medicine.
Whilst Britain is a country which is good at making its own laurel wreaths, it is also a country where those things which are normal features of being recognized as a member of the same species – homo sapiens – are withheld on cultural whim. Amnesty International’s yearly world report details some of the human rights breaches which Britain has actioned in 2021 – summary excerpt below (Amnesty International, 2021).
“The government response to COVID-19 raised human rights concerns, including in relation to health, immigration policies, domestic abuse and housing. Instances of racial discrimination and excessive force against protesters by the police were documented. Northern Ireland made progress on same-sex marriage and abortion, but full accountability for past violations remained unrealized. New licences for military exports to Saudi Arabia resumed. Bills on counter-terrorism and overseas military operations endangered human rights. Extradition proceedings against Julian Assange threatened the right to freedom of expression.”
Amnesty International, (2021), Amnesty International Report 2020/21: The State of the World’s Human Rights, Taken from internet 22.8.22: https://www.amnesty.org/en/wp-content/uploads/2021/06/POL1032022021ENGLISH.pdf
Whilst Britain has a habit of pointing the finger at other countries it often fails to recognise its own failures; here medicine and psychiatry are very much fields structured by privilege, and privilege has hardened such vertical hierarchies that populations exist sorted into economic ghettos. The people who exist within economic ghettos are vulnerable to abuse by the system of finance which serves those who exist outside of the economic ghettos.
This ultimately results in harms made real through impoverishments of what is native to the homo sapien as a social mammal, and through predatory practices which exploit the needs of people. Human rights is contested in Britain by heritage which subscribes to absolutist perspectives of governance, as explored in the previous section. As a country it has a long history of colonizing, controlling and exploiting populations across the globe, but this also includes onshore Britain where arguably colonisation practices first emerged.
Human rights as a concept directly clashes with the class/caste system which permeates Britain’s culture and social arrangements. Whilst the Magna Carta was realised in Britain it’s purpose was to realise rights for barons rather than the common person, and this two tier dynamic continues to resemble the social reality today. What kind of representation within a system an individual gets depends on their status, and their status is governed by finance and the opportunities which that finance offers them.
Although Habeas Corpus is still one of the few extant writs of the Magna Carta, we must recognise that – despite its centrality in law – it has been overtly suspended for certain populations at times (i.e. for the peoples of Ireland 1849), and defacto suspended for other populations by recession of the legal means (such as documentary evidences from the Windrush generations and representation by legal professionals by due process) from the individuals.
In terms of mental and physical health, this effects people through their representation by law, the therapeutic offerings that they get access to and the corrections which are made to their situation when misdeeds have befallen individuals. Britain is shaped by its economic inequalities and these economic inequalities translate the relationships between all administrative structures and the individual; it is the administrative structures which are the governance structures of given institutions, enterprises and functionaries in a society.
The epidemiology’s associated with inequities are well evidenced by the longitudinal work of people such as Sir Michael Marmot and Professors Pickett and Wilkinson.

In the psychiatric juncture the question of someone’s humanity is placed within a sort of Schroedinger box along with something toxic; a person is perceived to exist in a quantum state of being human and yet not human; it is only on scrutiny, when the box is opened that the question is given a firm answer; for the rest of the time their humanity and wellbeing is in an imagined reality.
I suggest in the psychiatric context (and others) something like this happens with people’s human rights – they are perceived to exist and be realised and also the converse. The human inside the box must deal with the superpositions which culture theorises for them.

Better representation of rights is given to corporations which get represented as a person in law apart from their culpability and involvements in harms or plain malfeasance (white collar crime) (Joseph, 1999; Salinger, 2013).
“Multinational Enterprises (MNEs)2 are very powerful entities in the current world order. Indeed, it is trite to note that the power of some MNEs outstrips the power of certain nation-states.3 In view of their vast economic power and ubiquitous presence, and consequent intrusion into many aspects of people’s lives, it is not surprising that MNE activity can and does occasionally impact detrimentally on the enjoyment of internationally recognised human rights. Corporate leaders traditionally deny that their activities have anything to do with human rights, as their operations are strictly concerned with ‘business’.4
This conservative view holds that business and human rights are separate disciplines that do not overlap.5 Indeed, this view is reflected in the general absence of human rights considerations from international business laws and institutions.6 However, there is no doubt that MNEs can and do perpetrate human rights abuses, like probably all entities. The effects of MNE abuse are, however, amplified by the inherent power of MNEs…MNEs are capable of inflicting serious human rights abuse. Present methods of imposing accountability on MNEs for such abuse are deficient. There is therefore a need for reform of the international human rights regime to counter defacto MNE impunity.”
Joseph, S. (1999). Taming the Leviathans: Multinational Enterprises and Human Rights. Netherlands International Law Review, 46(2), 171-203. doi:10.1017/S0165070X00002394
“In the 2003 independent documentary The Corporation, directors Mark Achbar and Jennifer Abbott overlay the behavioral criteria used for assessing and diagnosing psychopathy, as detailed in the Diagnostic and Statistical Manual of Mental Disorders, onto the business model of the generic American corporation: a lack of empathy, self-grandiosity, interpersonally and economically exploitative behavior, and a host other antisocial traits common among criminal psychopaths. The film, at the time of its release, foreshadowed a prevailing anticorporate sentiment that has come to define much of the last decade and its economic turbulence.
Mark Achbar and Jennifer Abbott’s assessment of the typical—and typically American—corporation as a psychopath is not some abstract metaphor or anthropomorphization of companies as living and breathing beings. Their profile defaults to 19th-century American case law that assesses the rights and responsibilities of a corporation as equal to those, as defined in the Fourteenth Amendment, of a real person.
This concept of corporate personhood, beginning with Supreme Court decisions as early as 1819 in civil cases such as Dartmouth College v. Woodward and, later, Santa Clara County v. Southern Pacific Railroad were initially rationalized on the basis that in cases of contract violation, corporations should have the same rights and legal recourse as private individuals, because the employees working for corporations do not forfeit their rights as citizens just because they are working in consolidation.
However, when moving in the opposite direction with respect to accountability and liability, the corporation is able to default back to an amorphous collective in which no single individual can bear responsibility on behalf of the group. In other words, the corporation has, by the very nature of this paradoxical design, achieved all of the rights of a private and sovereign person, yet in most cases bears few if any of the associated responsibilities.
Part of the problem rests in the fact that a corporation, while defined as a person in the technical sense, cannot be arrested, arraigned, cross-examined, or jailed in the same manner as a flesh-and-blood defendant. As a result, most cases of corporate misbehavior with respect to unsafe products and workplace practices tend to be mediated through civil remedies, including stand-alone and class-action lawsuits. Exceptions include cases where identifiable individuals within a corporation are found engaging in flagrantly illegal practices—such as wire fraud, contract fraud, and insider trading—under the auspices of carrying on business; they are typically charged with crimes that fall within the white-collar category.”
Page 219, Salinger, L. M. (2013). Encyclopedia of white-collar and corporate crime. Sage Publications
Medicine as a corporate enterprise has come to ‘medicate’ countless numbers of people and its increasingly financial governance has altered the values systems that embody outcomes. Examining the anthropology and history of the corporate and administrative systems which dominantly govern the world is helpful in realising the values which are baked in. The corporation as a legal entity has its provenance in the East India Company, limited in its liability and writ in it a heritage of plundering cultures (Nick, 2017) and peddling addiction across the world (Haq, 2000).
“The year 2000 was the 400th anniversary of the founding of the English East India Company. It was also the year that I came to work in the City of London, where the Company had been headquartered throughout its 275-year existence. Then and now, the City forms one of the major hubs of international finance…
One day, I walked further east, heading along Leadenhall Street, aiming to visit the site of the East India Company’s headquarters and then head back to work. I was in for a surprise. When I reached the corner of Leadenhall and Lime Street, where East India House had stood for over two hundred years, there was nothing – no sign, no plaque, nothing to mark the fact that this was the location where the world’s most powerful corporation had once been based.
In a country that is drenched in the culture of heritage, this absence puzzled me: why had this historic Company been so completely erased from the face of London? This book is an attempt to answer this question and, more importantly, to re-examine the meaning of the Company’s legacy for the global economy of the twenty-first century. As I delved deeper into this corporation from the Age of Enlightenment, it became clear that this was not just a thing of the past, but an institution whose practices were strikingly familiar.
The Company had pioneered the shareholder model of corporate ownership and built the foundations for modern business administration. With a single-minded pursuit of personal and corporate gain, the Company and its executives eventually achieved market dominance in Asia, ruling over large swathes of India for a profit. But the Company also shocked its age with the scale of its executive malpractice, stock market excess and human oppression.
For me, the parallels with today’s corporate leviathans soon became overpowering, with the Company outstripping WalMart in terms of market power, Enron for corruption and Union Carbide for human devastation. There are countless histories of the East India Company, yet none address its social record as a corporation. This is a gap that this book seeks to fill, recovering a sense of the ferocious struggles over corporate accountability that the Company generated in the eighteenth century.”
Page x, Robins, N., (2017). The Corporation That Changed the World: How the East India Company Shaped the Modern Multinational. Pluto Press.
“Through the dealings of the British East India Company, opium, traditionally used medicinally, became a non-medicinal business commodity during the late eighteenth and through-out the nineteenth centuries… The colonial drug laws applied a double standard, as they allowed the imperial authorities to appropriate revenue from the state-run opium monopoly, while pushing the private traders to become involved in the contraband trade.
The Indian opium trade flourished until the late nineteenth century, when China emerged as a major market for the supply of opium from India. By the end of the century, the colonial rulers progressively increased local consumption of intoxicating drugs in South Asia through the establishment of an official distribution system. Thus, the history of the drug trade in South Asia has a complex political background with numerous cross-regional connections.”
Haq, M. E. (2000). The Colonial Drug Trade. Drugs in South Asia, 11–35. doi:10.1057/9780333981436_2
In his book ‘The Corporation’, Professor of Law Joel Bakan has compared the behaviour of corporations to the The Hare Psychopathy Checklist, a set of criteria used for the determination psychopathy in individuals, to illustrate the harms which come by way of corporation (Bakan, 2012). When we do these kinds of comparison it helps us notionalise the outcomes of how corporations are functioning in our lives; it helps us take seriously the fact that corporations are awarded personhood whilst simultaneously recognising these organisational structures are not tied to the same responsibilities as a real person is.

It helps contextualise how a collective outcome of a line managed process may be constructed of a number of small capitulations – sometimes none of which amount to human rights violations – but which when enacted together bring about clear ethical and physical harms which if perpetrated by an individual would be prosecutable under the auspices of the law.
What is important to consider in this age is that it might be a false dichotomy to cast psychiatric harms exclusively in a patient-doctor divide but instead direct our attentions to the systems effects of agents (medics) being bound to corporate rubrics and values. In organisational terms the multinational corporation draws its behavioural dynamics from the origins of the East India Company which raises key questions about how collective organisational means of collaboration must be evolved to check harms which emerge out of the current configurations of enterprises in the world.
“‘”The language of business is not the language of the soul or the language of humanity,’ she says. ‘It’s a language of indifference; it’s a language of separation, of secrecy, of hierarchy.’ It ‘is fashioning a schizophrenia in many of us.” Psychology, as Roddick’s last comment suggests, may provide a better account of business executives’ dual moral lives than either law or economics. That is why we asked Dr. Robert Hare, a psychologist and internationally renowned expert on psychopathy, for his views on the subject.
He told us that many of the attitudes people adopt and the actions they execute when acting as corporate operatives can be characterized as psychopathic. You try ‘to destroy your competitors, or you want to beat them one way or another,’ said Hare, echoing Roddick and Barry, ‘and you’re not particularly concerned with what happens to the general public as long as they’re buying your product.’ Yet, despite the fact that executives must often manipulate and harm others in pursuit of their corporation’s objectives, Hare insists they are not psychopaths.
That is because they can function normally outside the corporation-‘they go home, they have a warm and loving relationship with their families, and they love their children , they love their wife, and in fact their friends are friends rather than things to be used.’ Businesspeople should therefore take some comfort from their ability to compartmentalize the contradictory moral demands of their corporate and noncorporate lives, for it is precisely this ‘schizophrenia,’ as Roddick calls it, that saves them from becoming psychopaths.
The corporation itself may not so easily escape the psychopath diagnosis, however. Unlike the human beings who inhabit it, the corporation is singularly self-interested and unable to feel genuine concern for others in any context. Not surprisingly, then, when we asked Dr. Hare to apply his diagnostic checklist of psychopathic traits below) to the corporation’s institutional character, he found there was a close match.
The corporation is irresponsible, Dr. Hare continue doing what they did before anyway. And in fact in many cases the fines and the penalties paid by the organization are trivial compared to the profits that they rake in.’56 Finally, according to Dr. Hare, corporations relate to others superficially -‘their whole goal is to present themselves to the public in a way that is appealing to the public [but] in fact may not be representative of what th[e] organization is really like.’
Human psychopaths are notorious for their ability to use charm as a mask to hide their dangerously self-obsessed personalities. For corporations, social responsibility may play the same role. Through it they can present themselves as compassionate and concerned about others when, in fact, they lack the ability to care about anyone or anything but themselves.”
Page 56, Bakan, J. (2012). The corporation: The pathological pursuit of profit and power. New York: Constable & Robinson.
The iatrogenic harm – medical problems caused by medicines and medics – has been normalised as ‘the price we have to pay for the modern management of disease’ (Page 1, Sharpe & Faden, 2009). This moral disengagement from the damaging effects of the decisions of companies and institutions is a problem in the face of the dignities and wellbeing which everybody deserves in their own life. The corporate management of countries and the wellbeing of their citizens is increasingly problematic in terms of health care (Page 96, Sharpe & Faden, 2009).
“The phrase ‘medical harm’ seems paradoxical. It defies our expectations about medicine; our expectations that medicine will benefit, rather than harm us and that individual and institutional providers will improve rather than diminish our health. But iatrogenic illness – literally, illness that is ‘induced by the physician’ – has come to be recognized as a significant source of patient risk. In the United States, it has been estimated that during hospitalization, as many as a third of patients suffer from complications related to their medical or nursing care.’ Between 5% and 13% of hospital admissions result from the adverse effects of diagnosis or treatment.2
The 1991 Harvard Medical Practice Study concluded that almost 70% of iatrogenic complications are preventable and affect more than 1.3 million hospitalized patients annually.’ During the fee for service era, patients were believed to be at considerable risk for unnecessary treatments.4 Today, there is growing concern regarding the risks associated with economically-motivated denials of necessary care.5
In the last half of the twentieth century, attention to the problem of medically induced illness in the United States has come from a number of sources including the medical and legal professions, federal agencies and consumer advocacy groups.
It was in the 1950s and 1960s, after the enormous post-war expansion in pharmacological therapies, that the occurrence of iatrogenic complications – particularly adverse drug reactions – began to receive attention in the medical literature. From the professional point of view at this time, iatrogenic adverse effects were regarded as the inevitable price of medical progress; ‘the price we must pay for the modern management of disease,’6
Sharpe, V. A., & Faden, A. I. (2009). Medical Harm: Historical, Conceptual And Ethical Dimensions Of Iatrogenic Illness. Cambridge, Gbr, Cambridge University Press. Http://Public.Ebookcentral.Proquest.Com/Choice/Publicfullrecord.Aspx?P=4638246. Page 1
“Although the fiduciary model continues to be the dominant model in both medical ethics and law, it is increasingly strained by a changing health care system in which physicians are held accountable to interests other than those of the patient. As physicians become more accountable to corporate agents and, in particular, accountable for their financial performance, the fiduciary model will press them to express their obligations of beneficence and nonmaleficence in active advocacy for the interests of patients.54 The fiduciary model will also be challenged to address the conditions under which the interests of the patient may be justifiably weighed against the legitimate interests of others.55”
Sharpe, V. A., & Faden, A. I. (2009). Medical Harm: Historical, Conceptual And Ethical Dimensions Of Iatrogenic Illness. Cambridge, Gbr, Cambridge University Press. Http://Public.Ebookcentral.Proquest.Com/Choice/Publicfullrecord.Aspx?P=4638246. Page 96
The issue of medicine related harms is especially prevalent in the context of psychiatry as levels of iatrogenic harm stand out and the institutional approaches to psychological wellbeing seem to be systematically failing to address the problems (Meadows et al, 2019; Mulder, Rucklidge & Wilkinson, 2017).
“Australian mental health care expenditure per-person has increased in real terms through two decades by nearly 100%, and by 30% in the last decade (Meadows et al., 2018). The National Mental Health Strategy and the National Action Plan for Mental Health have guided large-scale mental health care investments, including the Better Access to Mental Health Care (‘Better Access’) programme, greatly increasing psychological services delivery (Jorm, 2018).
But, Australian community health survey findings suggest no change from 2001 to 2014 in prevalence of the higher scores on the Kessler 10 instrument commonly associated with clinically significant mental health problems (Meadows So, as others have highlighted in this journal, we have a seeming paradox to resolve (Mulder et al., 2017): why has more expenditure and more treatment not led to an identifiable decrease in prevalence? This is unlikely to have any one explanation.
Contributory causes may include increasing inequality driving an underlying prevalence increase (Wilkinson and Pickett, 2018), possibly exacerbated by social, demographic, cultural and environmental changes in the cities (O’Hanlon, 2018), where most Australians live. These might have important implication for policy, This paper will focus on healthcare planning, delivery and education, where there have been proposals for major services redesign and reorientation (Van Os et al., 2019) and the suggestion that ‘We need to, at the least, consider whether our current mental health systems might be causing unintentional harm in some areas.
It is possible that in order to achieve better outcomes, we need to do less, not more’ (Mulder et al., 2017). We suggest a possible contributing mechanism that might indeed be causing unintentional harm, or iatrogenesis, and so contributing to this worrying situation. As a During the mid-1970s, the Austrian social theorist Ivan lllich (Hartch, 2015), influential then in social work, education and sociology, provided a critical perspective on directions being taken by modern medicine.
Proposing that medicalisation of life problems had extended beyond the bounds of conditions where there was convincing evidence that medicine could help, and that in various ways the medical establishment was a source of disability as much or more than of therapeutic benefit, lllich (1976) expanded the concept of iatrogenesis or physician-caused illness beyond prior usage, suggesting a threefold nature for iatrogenesis: clinical, social and cultural – of which our summary follows. ”
Meadows GN, Prodan A, Patten S, Shawyer F, Francis S, Enticott J, Rosenberg S, Atkinson JA, Fossey E, Kakuma R. (2019 ) Resolving The Paradox Of Increased Mental Health Expenditure And Stable Prevalence. Aust N Z J Psychiatry. ;53(9):844-850. Doi: 10.1177/0004867419857821. Epub 2019 Jun 25. Pmid: 31238699; Pmcid: Pmc6724452.
“Psychiatric services in developed countries face a dilemma: despite increased effort and resources directed at mental health problems, measures of psychological distress appear to be worsening. In New Zealand, for example, mental health funding rose from NZD1.1 billion in 2008/2009 to nearly NZD.4 billion in 2015/2016 (New Zealand Ministry of Health data). The number of psychiatrists and psychologists almost doubled from 2005 to 2015. More people than ever are receiving mental health treatment.
For example, the Auckland District Health Board reported an increase from around 2000 crisis referrals in 2010 to more than 6000 in 2015. More people are taking psychotropic medications than ever recorded. PHARMAC data in 2015 reveal that 13.7% of all New Zealanders have been dispensed antidepressants and 3.1% antipsychotics. Both rates have increased by more than 50% in the past decade (Ministry of Health Pharmaceutical Collection).
Despite all this effort, objective measures of community mental health have not been improving and in most cases are worsening. According to the New Zealand Health Survey, the number of children suffering from psychiatric problems has more than doubled between 2008 and 2013. The percentage of the adult population with high psychological distress (K10 3= 12) has increased from 4.5% in 2011 to 6.8% in 2016. There has been a fourfold increase in people on disability benefits due to a mental illness from 1991 to 2011 (Statistics New Zealand Annual Reports). The suicide rate remains stubbornly high.
These data lead to an obvious question: if the treatments we provide are effective, then increasing them should lead to a decrease in measures of community mental disorder rather than the increase we appear to be experiencing. In other words, if our treatments work shouldn’t we have fewer people presenting in crisis, less people on a disability benefit due to mental illness, a reduction in community measures of psychological distress and a decrease in the suicide rate?”
Mulder R, Rucklidge J And Wilkinson S (2017) Why Has Increased Provision Of Psychiatric Treatment Not Reduced The Prevalence Of Mental Disorder? Australian And New Zealand Journal Of Psychiatry 51: 1176–1177.
The field of psychiatry is especially problematic because the voice and experience of the individual is devalued from the outset; they are overshadowed by the use of ephemeral nature of medical diagnoses, shifting regimes of powerful and intoxicating prescription drugs, by the vertical power relationships of the medic to patient, and by the diagnostic identity that is given them.
The effects of drugs are not uncommonly mistaken for the diagnosis (Bahiya & Sujith 2017; Narsi et al, 2010), and when this does occur it sets up the possibility of sociological cascades happening. When the behaviour of individuals has been altered by drugs those around them can perceive the individual as ‘other’, as ‘different’ and/or ‘abnormal’ resulting in a positive feedback loop whereby more and more ‘medical interventions’ are heaped on them.
We can work a basic thought experiment by imagining drinking alcohol when going into a sociological environment where sobriety is expected; I suggest that all the behavioural actions which might transpire are possible to come about when someone is acting under the influence of a strong psychoactive drug. The public messaging which has been associated with psychoactive drug use and behaviours associated with psychoactive drug use are powerfully indoctrinated with notions like ‘sociological defection’; this has been heavily reinforced through ideological movements such as ‘the war on drugs‘.
“For more than half a century, drug induced Parkinsonism (DIP) has captured the attention of the physicians and researchers alike. More and more drugs underwent extensive scrutiny and causal agents were penned down from notorious antipsychotics [1] to more innocent anti-arrhythmic agents DIP can be defined as reversible development of parkinsonian syndrome in patients treated with drugs which impair dopamine function [23], Parkinsonian syndromes includes symptom complexes such as tremor, rigidity and bradykinesia in addition to loss of postural reflexes and freezing [24]. Time for recovery from DIP may vary from days to years after offensive drugs are withdrawn [25], Though reversible, in significant amount of individuals even after withdrawing the causal agents the symptoms persisted [26-29]. This may indicate ongoing toxicity, irreversible deficit or unmasking underlying parkinsonism syndrome.”
Bahiya S, Sujith O. (2017) Drug Induced Parkinsonism: An Overview. Open Access J Neurol Neurosurg.; 3(4): 555620. Doi: 10.19080/Oajnn.2017.03.555620
“The side effects commonly seen with conventional antipsychotics include sedation, anticholinergic effects, extrapyramidal symptoms (EPS), orthostatic hypotension, weight gain, photosensitivity, and elevated prolactin levels. Sedation and the feeling of tiredness are very common with all antipsychotics.3 Extra pyramidal symptoms (EPS) are neurological disturbances caused by antipsychotics in the area of the brain that controls motor coordination. The antipsychotics drug can produce symptoms like Parkinson’s disease. They cause Parkinson like symptoms (parkinsonism) that include muscle stiffness, rigidity, tremor, drooling, and a “masklike” face…
Akathisia is another form of EPS characterized as a subjective sense of restlessness accompanied by fidgeting, inability to sit still, nervousness, muscle discomfort, and agitation. Use of propranolol , a betablocker, may be helpful…Tardive dyskinesia is a potential adverse reaction from antipsychotic medications. It is a late-onset abnormal involuntary movement disorder. It is a potentially irreversible condition with symptoms that commonly include “pill-rolling” movements of the fingers, darting and writhing movements of the tongue, lip puckering, facial grimacing, and other irregular movements. The risk of TD is increased the longer the person has been taking the antipsychotic and this risk also increases with age…
Classical tardive dyskinesia is characterized by involuntary lip smacking and pursing, movement of the tongue side-to-side (bon-bon sign), tongue protrusion (Fly-catcher’s tongue), chewing movements, respiratory dyskinesia (diaphragm and intercostal involvement), pelvic thrusting, choreiform limb movements, tapping and side-to-side foot movements, and marching in place. The dyskinesia appears to affect the lower face more than the upper face. It has been suggested that these movements can be Tardive tic may develop in a small number of patients on chronic neuroleptic therapy, which resemble Gilles de la Tourette syndrome (make repeated and uncontrolled (involuntary) movements and sounds (vocalizations) called tics.).
These patients demonstrate spontaneous vocal and motor tics. These include barking, clicking, grunting and verbalization. Tardive akathisia is described as a subjective restlessness or need to move, which may occur early in the course of Neuroleptic therapy. Some of the stereotyped motor Tardive akathisia is described as a subjective restlessness or need to move, which may occur early in the course of Neuroleptic therapy.
Some of the stereotyped motor movements attributed to TD, including repetitive touching of the forehead and scalp, crossing and uncrossing of legs, pacing and body rocking, may be due to akathisia. 1) Can’t sit still 2) Inner feeling of restlessness/anxiety/discomfort 3) Restlessness usually more severe when trying to fall asleep 4) Compulsion to keep moving 5) Itchy, painful burning tingling skin 6) Depression that never existed before 7) Suicidal thoughts/actions which never existed before”
Narsi Reddy, K., Banji, D., Banji, O.J., Reddy, J.A., & Swetha, M. (2010). An Overview Of Tardive Dyskinesia. International Journal Of Pharmaceutical Sciences Review And Research, Volume 4, Issue 3, September – October 2010; Article 019 Issn 0976 – 044x
The status placed in the medic and medical institution gives them disproportionate authority calling on long heritage of impunity of protected professions well noted in jurisprudence (Finnis, 2011). It is common for institutions to deal with misdemeanors ‘inhouse’ away from the public gaze in an effort to protect the integrity of the institution. For example Finnis argues that “if an unjust stipulation is, in fact, homogeneous with other laws in its formal source, in its reception by courts and officials, and in its common acceptance, the good citizen may (not always) be morally required to conform to that stipulation to the extent necessary to avoid weakening ‘the law’”.
“It may be the case, for example, that if I am seen by fellow citizens to be disobeying or disregarding this ‘law’, the effectiveness of other laws, and/or the general respect of citizens for the authority of a generally desirable ruler or constitution, will probably be weakened, with probable bad consequences for the common good. Does not this collateral fact create a moral obligation? The obligation is to comply with the law, but it should not be treated as an instance of what I have called ‘legal obligation in the moral sense’.
For it is not based on the good of being law-abiding, but only on the desirability of not rendering ineffective the just parts of the legal system. Hence, it will not require compliance with unjust laws according to their tenor or ‘legislative intent’, but only such degree of compliance as is necessary to avoid bringing ‘the law’ (as a whole) ‘into contempt’. This degree of compliance will vary according to time, place, and circumstance; in some limiting cases (e.g. of judges or other officials administering the law) the morally required degree of compliance may amount to full or virtually full compliance, just as if the law in question had been a just enactment.
So, if an unjust stipulation is, in fact, homogeneous with other laws in its formal source, in its reception by courts and officials, and in its common acceptance, the good citizen may (not always) be morally required to conform to that stipulation to the extent necessary to avoid weakening ‘the law’, the legal system (of rules, institutions, and dispositions) as a whole. The rulers still have the responsibility of repealing rather than enforcing their unjust law, and in this sense have no right that it should be conformed to. But the citizen, or official, may meanwhile have the diminished, collateral, and in an important sense extra-legal obligation to obey it.”
Finnis, J. (2011). Natural Law And Natural Rights (Clarendon Law Series). Oxford University Press. Page 361
This example demonstrates how within institutional spaces there are situations where what is right is overridden by the drive for conformity and authority. We can see this kind of principle of illustrated in situations such as Parliamentary and Presidential Privilege/Immunity where parliamentarians (etc) are granted full immunity from legal prosecution, both civil prosecution and criminal prosecution, in the course of the execution of their official duties. This kind of impunity can be related back to the anthropological records of Thomas Hobbes in his ‘Leviathan’ where he suggests infallibility upon the notion of an absolute sovereign contrasting to Lockean perspectives.
A problematisation of parliamentary privilege is offered by Dr Adam Tucker, Lecturer in Law at the University of Manchester who teaches and researches in the fields of Constitutional Law and Constitutional Theory: “Parliamentary privilege undermines the rule of law. Specifically it undermines the requirement, which is central to the rule of law, that the law be general. Even worse: it undermines that requirement in a particularly worrying way because it mainly (although not only) has the effect of excusing members of the political elite from conformity with the law”.
(Parliamentary Privilege Consultation: Response of Dr Adam Tucker, Parliamentary Privilege and Constitutional Principle 2. 3. 4. 5. 6., Retrieved from internet 6.1.23: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment
_data/file/79391/PPC_Response_Dr_Adam_Tucker.pdf)
In a related way I argue that the corporate configuration of medicine and institutions undermine the core aims they arise from resulting in human rights harms and violations due to opacity and impunity. If we take as our starting point for medicine the intervention of illness, it follows that the causes of ill health must be available for scrutiny and include the systems and ecologies which deploy interventions.
Taking into consideration the fact that the diagnoses are often scientifically little understood (American Psychiatric Association, 2017), we arrive at the point where an investigation must be launched to scrutinising the governing influences of medicine. In the psychiatric juncture this necessarily must involve the questioning of cultural values at play in society, the economic configuration of the enterprises involved in delivering the tools which are sanctioned as interventions and the legal configurations which interfere with science as the foundation of medicine.
“The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM) is a classification of mental disorders with associated criteria designed to facilitate more reliable diagnoses of these disorders. With successive editions over the past 60 years, it has become a standard reference for clinical practice in the mental health field. Since a complete description of the underlying pathological processes is not possible for most mental disorders, it is important to emphasize that the current diagnostic criteria are the best available description of how mental disorders are expressed and can be recognized by trained clinicians.”
American Psychiatric Association (2017). Diagnostic And Statistical Manual Of Mental Disorders: Dsm-5. Arlington, Va, American Psychiatric Association. Preface
Dealing with the latter point of science as the foundation of medicine, Jureidini and McHenry offer a powerful critique in their book ‘The Illusion of Evidence Based Medicine’. As established academics they have sought to criticise orthodox medicine as having become influenced by unaccountable multinational companies which enjoy the impunity of their corporate structure.
Drawing on court records where the legal system has forced companies to release information vital to determining the outcome of various court cases and examining the highly financialised make up of scientific reporting, they argue that certain correctives must be made to restore the scientific foundations essential to informed medicine.

The multimodal perception involved in arriving at understandings of mental illness give harbour to a range of social contagion – group behaviours which involve emotive ideas and feelings spreading spontanously through networks of people. Psychiatry has become a catch all for perceptions of people considered as ‘other’ evoking in some situations dehumanising sociological responses (Fiske, 2012).
“Mental illness subtypes. People with mental illness are stigmatized as a whole (Corrigan. 2004: Link. Yang. Phelan. & Collins. 2004). What’s more, as SCM shows, varieties of mental illnesses carry distinct stereotypes in society’s mind. After undergraduates listed common kinds of mental illnesses, another sample rated how society views these subtypes.3
Although people with mental illness in general may be either pitied or feared, the different types appear distinct to lay people (see Figure 2). For this sample, people with attention deficit disorder or eating disorders seemed “normal,” both competent and warm. Probably many of these undergraduates were, or knew people who were, living with these issues. For them, the most stigmatized mental disorders, those without redeeming features, included people with schizophrenia or generic psychopathology. These most extreme mental illness images are probably what comes most often to mind when people imagine someone with mental illness as unreliable.
More mixed responses target people with depression, bipolar disorder, and obsessive-compulsive disorder, who are seen collectively as competent but not warm and trustworthy. This view fits the romantic and unrealistic mad-genius image. The other mixed cluster contains people with mental disabilities, such as what our respondents termed mental retardation and Downs Syndrome, people viewed as incompetent but warm and trustworthy.
These images suggest that some mentally ill people will be stigmatized with disgust and contempt—for example, schizophrenics—whereas people with bipolar disorder may be admired as brilliant but mistrusted. Both clusters, being in the low-warmth part of the space, may be feared and resented, if these data fit earlier such instances (Fiske et al., 2002). In contrast, other types of mental illness may be greeted as trustworthy and even familiar, as is the case with eating disorders (competent, so respected, even perversely admired) and mental retardation (not competent, so pitied).”
Fiske S. T. (2012). Warmth And Competence: Stereotype Content Issues For Clinicians And Researchers. Canadian Psychology = Psychologie Canadienne, 53(1), 14–20. Https://Doi.Org/10.1037/A0026054
Professor Fiske’s research at Princeton University has focused on mapping social cognition and varieties of dehumanizing responses which are commonly associated with stereotypes. She and her colleagues developed the Stereotype Content Model which elucidates various aspects of how people are humanized and dehumanized according to the labels which they are seen through. Her research is telling in respect to psychiatric labels and the behaviours they promote in others, but also it is revealing in that it shows that certain groups are dehumanised three orders of magnitude more than other social groupings resulting in them being called ‘extreme outgroups’.
People who lack a place of shelter, homeless people, are a social grouping which encounter mental illness disproportionately more in comparison to other groups and which face prejudices at levels way in excess than other social groupings do – homelessness is a stereotype that is a part of extreme out groups. Fiske’s work helps us analyse the cultural prejudices which significantly influence the way people are treated and clarify how sociological harms and dehumanization play a role in mental health.

“this is a representative sample survey we did a while back and the names of the groups are the names that people supply for us, so if you find some of them offensive it’s because these are the names that people give us for the different groups; and what you see in a cluster analysis is in a low low part of the space are some of the groups I mentioned before. Homeless people are three standard deviations out from everybody else in the space so we have to take them out of the analysis or else they distort it – but if you don’t want to talk about people who are out of the human clusters that’s where homeless people are” (Transcript excerpt 15 minutes 11 seconds)
Susan T. Fiske, Varieties of (De)Humanizing – Divided by Status & Competition, Retrieved from internet 14.01.2023: www.youtube.com/watch?v=f–dDx0q6so
Dehumanization processes lay the ground work for moral disengagement and perpetration of violence on targets. Bearing that in mind we can look at the statistics of homeless populations and find that they are are 13 times more likely to experience violent attacks than a member of the general public and that just over half of the sample, 52% had experienced violence in the past year, in contrast to 4% of the general population (Crisis, 2005). Taking this as a litmus on how extreme outgroups are treated, we have to ask the question as to how certain mental health diagnoses dehumanize individuals and ask whether the way they are treated include culturally normalized forms of violence.
In the light of this, is there a link between violence, trauma and mental health diagnoses ? To offer some healthy cultural provocations, I have been asking myself whether the way that elderly people are warehoused constitutes culturally normalized forms of violence ? What are the ways which violence towards women are disguised as issues which as a culture allow us to morally disengage from the horrific statistics ? In what ways are expressions of violence towards non-heterosexual individuals swept under carpets out of sight and mind ? How does our culture subtly sanction forms of violence on people of colour ? Why are expressions of violence against migrant populations hailed as acceptable in our media ?
Newburn, T. & Rock, P. (2005) Living in Fear: Violence and Victimisation in the Lives of Single Homeless People. London: Crisis. http://www. crisis.org.uk/data/files/publications/LivingInFear_full.pdf
Is Mental Illness a Cultural Marker of Human Rights Violations ?
Given that mental health problems are on the increase, and that drug approaches seem to be failing to resolve the issues beyond offering a basic dissociative intoxication (commonly with progressing side effects), are we now at a juncture where we need to ask if the mental health crises that we are facing is a result of sociological configurations ? Are mental health crises hallmarks of the damages which come about when human rights are impinged by social arrangements that exploit and/or harm the human ?
If we consider that human rights refers not just to legal definitions of what is accorded to individuals in a just society but also that they correlate with what are necessary provisions for humans as social mammals to be healthy and functional in a society, as a society, a range of questions opens up. These questions include scrutinising the prevalence of support for punitive policies in order to govern society.
This view of mental health demands looking at forms of poverty and the punishments which are placed on populations for not having sufficient forms of wealth to participate in cultural activities. It orients an examination of issues such as addiction, homelessness, racism, sexism, homophobia and bullying in terms of clear harms which are embodied responses to unacknowledged justice issues and the disenfranchised grief they cause (Doka, 2002). It also positions exposure to environmental toxins such pesticides and industrial pollutants as a human rights issue that effects the behaviour, mood and cognition of populations – i.e. a company and/or a person is violating someone’s human rights by depriving them of health.
“Disenfranchised grief can be defined as the grief experienced by those who incur a loss that is not, or cannot be, openly acknowledged, publicly mourned or socially supported. Isolated in bereavement, it can be much more difficult to mourn and reactions are often complicated. The concept of disenfranchised grief recognises that societies have sets of norms – in effect, ‘grieving rules’ – that attempt to specify who, when ,where, how, how long, and for whom people should grieve.
These grieving rules may be codified as personnel policies. For example, a worker may be allowed a week off for the death of a spouse or child, three days for the loss of a parent or sibling. Such policies reflect the fact that each society defines who has a legitimate right to grieve, and these rights correspond to relationships, primarily familial, that are socially recognised and sanctioned. However these grieving rules may not correspond to the nature of attachments, the sense of loss, or the feelings of survivors and hence their grief is disenfranchised. In our society this may occur for a number of reasons”
Are we overwhelmingly medicating for social abuses and exposure to negative externalities of corporate business ? With a sociopathic economy at work is it not right to question corporate medicine and the roles it plays in peoples lives ? Is it not reasonable to theorise psychological damages on populations, be they those in prisons or care facilities; should children who experience the world as constricted of landscapes to play and socialise in be labelled as sick or should the society be ? Should human rights be understood as corresponding to critical components of health ?
I would argue yes.
References:
- American Psychiatric Association (2017). Diagnostic And Statistical Manual Of Mental Disorders: Dsm-5. Arlington, Va, American Psychiatric Association. Preface
- Alston, P (2019), Do Human Rights Investigations Matter ? The Case of the UN Special Rapporteur on Extreme Poverty’, October 16, 2019 at NYU School of Law with Philip Alston, John Norton Pomeroy Professor of Law, Margaret Satterthwaite Professor of Clinical Law, and César Rodríguez-Garavito, Founding Director of Program on Global Justice and Human Rights
- Amnesty International, (2021), Amnesty International Report 2020/21: The State of the World’s Human Rights, Taken from internet 22.8.22: https://www.amnesty.org/en/wp-content/uploads/2021/06/POL1032022021ENGLISH.pdf
- Bahiya S, Sujith O. (2017) Drug Induced Parkinsonism: An Overview. Open Access J Neurol Neurosurg.; 3(4): 555620. Doi: 10.19080/Oajnn.2017.03.555620
- Bakan, J. (2012). The corporation: The pathological pursuit of profit and power. New York: Constable & Robinson.
- Bentham J. (2011). The Panopticon Writings. Verso
- Committee J. F. (2022). Bnf 83 (british national formulary) march 2022 (83th ed.). Pharmaceutical Press
- Dickinson T. (2016). ‘Curing Queers’ : Mental Nurses And Their Patients 1935-74. Manchester University Press
- Kenneth J Doka PhD (1999) Disenfranchised grief, Bereavement Care, 18:3, 37-39, DOI: 10.1080/02682629908657467
- Edwin Black (9 November 2003). “Eugenics and the Nazis – the California connection”. San Francisco Chronicle. Retrieved 19.12.2022: https://www.sfgate.com/opinion/article/Eugenics-and-the-Nazis-the-California-2549771.php
- El-Hai, J. (2005), The Exiled Kennedy. The Independent. Retrieved 29.12.22: https://www.independent.co.uk/news/world/americas/the-exiled-kennedy-486688.html
- Finnis, J. (2011). Natural Law And Natural Rights (Clarendon Law Series). Oxford University Press. Page 361
- Fiske S. T. (2012). Warmth And Competence: Stereotype Content Issues For Clinicians And Researchers. Canadian Psychology = Psychologie Canadienne, 53(1), 14–20. Https://Doi.Org/10.1037/A0026054
- Fiske S. T. (2012) (Varieties of (De)Humanizing – Divided by Status & Competition, Retrieved from internet 14.01.2023: www.youtube.com/watch?v=f–dDx0q6so
- Friedlander W. J. (2001). The history of modern epilepsy : the beginning 1865-1914. Greenwood Press. Page 111
- Goodwin, D. K, (1987) The Fitzgeralds and the Kennedys, Simon and Schuster, Page 640
- Haq, M. E. (2000). The Colonial Drug Trade. Drugs in South Asia, 11–35. doi:10.1057/9780333981436_2
- Joseph, S. (1999). Taming the Leviathans: Multinational Enterprises and Human Rights. Netherlands International Law Review, 46(2), 171-203. doi:10.1017/S0165070X00002394
- Jureidini J, McHenry LB. The illusion of evidence based medicine. BMJ. 2022 Mar 16;376:o702. doi: 10.1136/bmj.o702. PMID: 35296456.
- Larson K. C. (2016). Rosemary: The Hidden Kennedy Daughter. Mariner Books / Houghton Mifflin Harcourt.
- Leamer L. (2002). The kennedy men : 1901-1963 : the laws of the father (1st Perennial). Perennial.
- Lekka V. (2015). The neurological emergence of epilepsy : the national hospital for the paralysed and epileptic (1870-1895). Springer. Page 59
- Locke, J. (1955). Of Civil Government: Second treatise. Chicago: Henry Regnery Co. Chapter IV
- Kaculini, C. M, Tate-Looney, A. J, Seifi, A. The History of Epilepsy: From Ancient Mystery to Modern Misconception. Cureus. 2021 Mar 17;13(3):e13953. doi: 10.7759/cureus.13953. PMID: 33880289; PMCID: PMC8051941.
- MacGregor, N., (2006) “The whole world in our hands”, in Art and Cultural Heritage: Law, Policy, and Practice, pp. 384, ed. Barbara T. Hoffman. Cambridge University Press. ISBN 0-521-85764-3
- Meadows GN, Prodan A, Patten S, Shawyer F, Francis S, Enticott J, Rosenberg S, Atkinson Ja, Fossey E, Kakuma R. (2019 ) Resolving The Paradox Of Increased Mental Health Expenditure And Stable Prevalence. Aust N Z J Psychiatry. ;53(9):844-850. Doi: 10.1177/0004867419857821. Epub 2019 Jun 25. Pmid: 31238699; Pmcid: Pmc6724452.
- Metzl J. (2010). The Protest Psychosis : How Schizophrenia Became A Black Disease. Beacon Press.
- Mulder R, Rucklidge J And Wilkinson S (2017) Why Has Increased Provision Of Psychiatric Treatment Not Reduced The Prevalence Of Mental Disorder? Australian And New Zealand Journal Of Psychiatry 51: 1176–1177.
- Narsi Reddy, K., Banji, D., Banji, O.J., Reddy, J.A., & Swetha, M. (2010). An Overview Of Tardive Dyskinesia. International Journal Of Pharmaceutical Sciences Review And Research, Volume 4, Issue 3, September – October 2010; Article 019 Issn 0976 – 044x
- Newburn, T. & Rock, P. (2005) Living in Fear: Violence and Victimisation in the Lives of Single Homeless People. London: Crisis. http://www. crisis.org.uk/data/files/publications/LivingInFear_full.pdf
- O’Brien, G. (2004). Rosemary Kennedy: the Importance of a Historical Footnote. Journal of Family History, 29(3), 225–236. doi:10.1177/0363199004266849
- Parliamentary Privilege Consultation: Response of Dr Adam Tucker, Parliamentary Privilege and Constitutional Principle 2. 3. 4. 5. 6., Retrieved from internet 6.1.23: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/79391/PPC_Response_Dr_Adam_Tucker.pdf
- Podrabinek A. (1980). Punitive medicine (1st ed.). Karoma.
- Rang H. P. Dale M. M. Flower R. J. & Henderson G. (2016). Rang and dale’s pharmacology (Eighth). Elsevier Churchill Livingstone. Page 549 to 555
- Robins, N., (2017). The Corporation That Changed the World: How the East India Company Shaped the Modern Multinational. Pluto Press.
- Robinson J. (2016), In The Family Way : Illegitimacy Between The Great War And The Swinging Sixties. Thorpe, Leicester, Chapter 1
- Ronald Kessler – The Sins of the Father_ Joseph P. Kennedy and the Dynasty He Founded-Grand Central Publishing (2012)
- Salinger, L. M. (2013). Encyclopedia of white-collar and corporate crime. Sage Publications
- Sharpe, V. A., & Faden, A. I. (2009). Medical Harm: Historical, Conceptual And Ethical Dimensions Of Iatrogenic Illness. Cambridge, Gbr, Cambridge University Press. Page 96
- Solzhenit︠s︡yn, A., (2018). The Gulag Archipelago 1918-56: An Experiment in Literary Investigation, Vintage Classics.
- The Eugenics Record Office at Cold Spring Harbor Laboratory (1910-1939). The Embryo Project Encyclopedia. Retrieved 19.12.2022: https://embryo.asu.edu/pages/eugenics-record-office-cold-spring-harbor-laboratory-1910-1939
- Tully, J., & Skinner, Q. (2009). Approach To Political Philosophy. Cambridge, Gbr, Cambridge University Press. Http://Public.Ebookcentral.Proquest.Com/Choice/Publicfullrecord.Aspx?P=4638354. P 29
- Wise S. (2013), Inconvenient People : Lunacy Liberty And The Mad-Doctors In Victorian England. Vintage Books, Preface